

Renal outcomes of STOP-IgAN trial patients in relation to baseline histology (MEST-C scores)
- PMID: 30453889
- PMCID: PMC6245781
- DOI: 10.1186/s12882-018-1128-6
Renal outcomes of STOP-IgAN trial patients in relation to baseline histology (MEST-C scores)
Abstract
Background: The Oxford classification of IgA nephropathy (IgAN) defines histologic criteria (MEST-C) that provide prognostic information based on the kidney biopsy. There are few data on the predictive impact of this classification in randomized clinical trial settings.
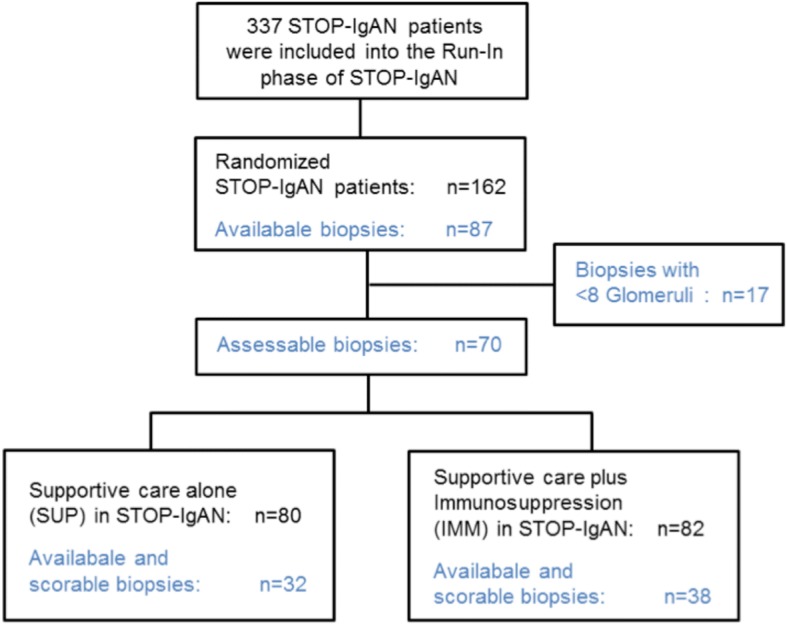
Methods: We performed an exploratory analysis of MEST-C scores in 70 available renal biopsies from 162 randomized STOP-IgAN trial participants and correlated the results with clinical outcomes. Analyses were performed by researchers blinded to the clinical outcome of the patients. Biopsies had been obtained 6.5 to 95 (median 9.4) months prior to randomization.
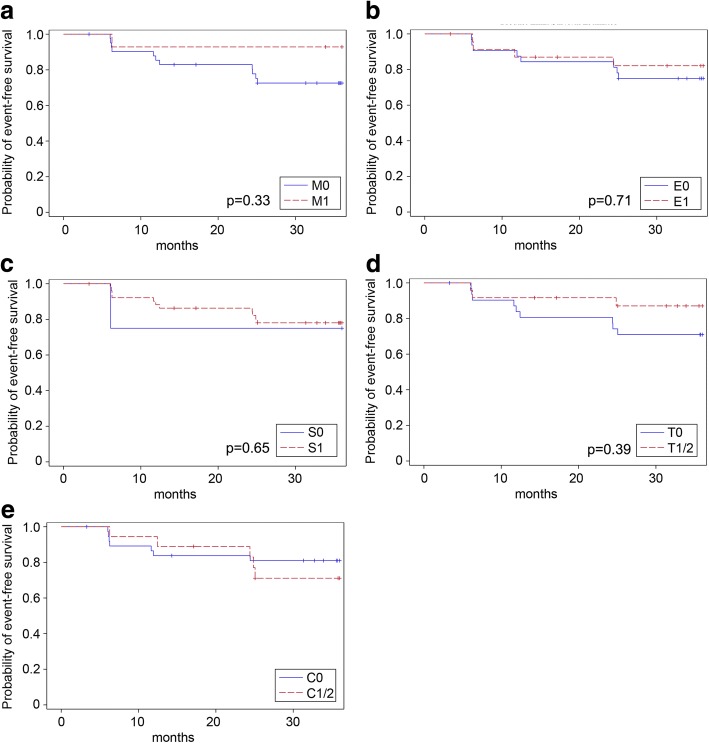
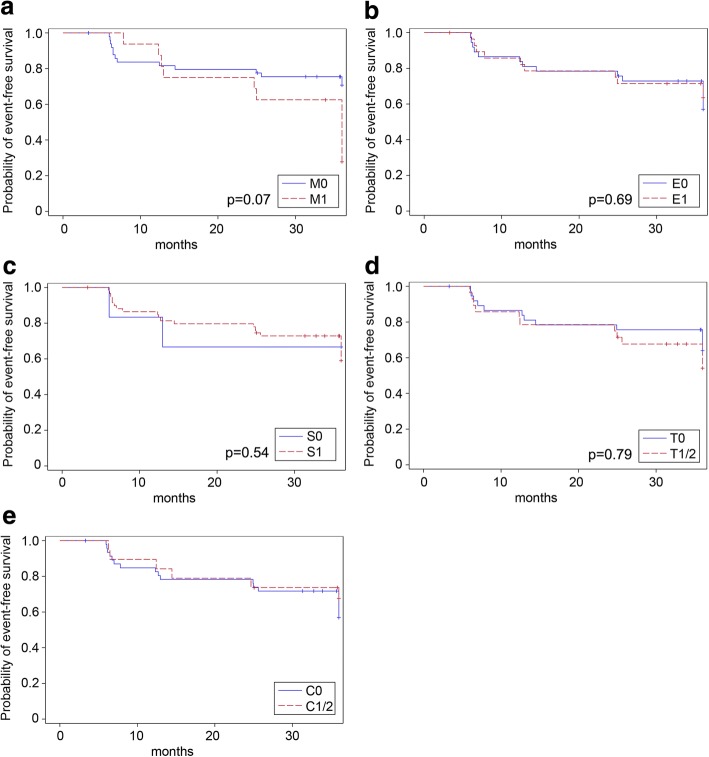
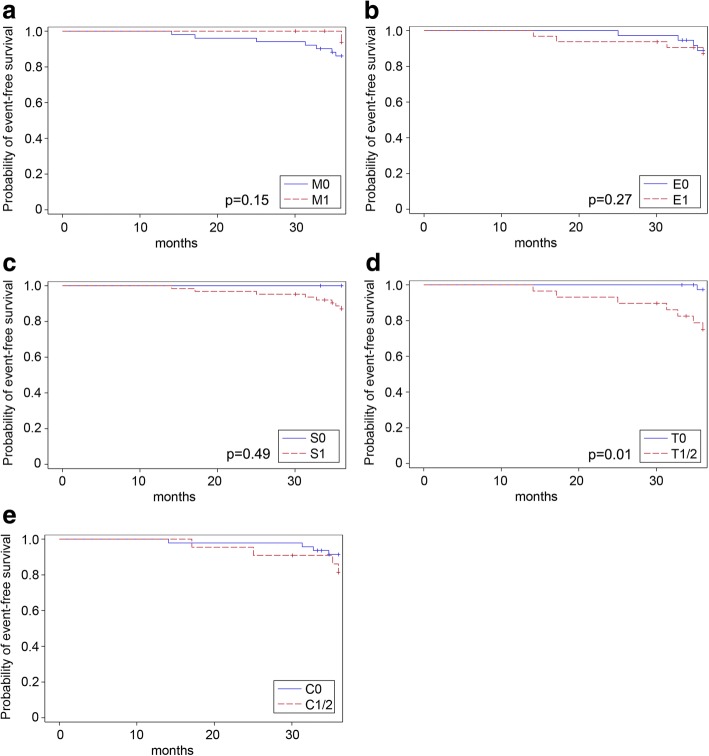
Results: Mesangial hypercellularity (M1) associated with higher annual eGFR-loss during the 3-year trial (M1: - 5.06 ± 5.17 ml/min/1.73 m2, M0: - 0.79 ± 4.50 ml/min/1.73 m2, p = 0.002). An M0-score additionally showed a weak association with full clinical remission, whereas the percentage of patients losing ≥15 ml/min/1.73 m2 over the 3-year trial phase was higher among those scored as M1. Among patients with additional immunosuppression, ESRD occurred more frequently in patients when tubulointerstitial fibrosis (T1/2) was present (T1/2 = 33%, T0 = 0%, p = 0.008). In patients receiving supportive care only, ESRD frequencies were similar (T1/2 = 18%, T0 = 7%, p = 0.603). At randomization, eGFR was significantly lower when tubulointerstitial fibrosis was present (T1/2: 45.2 ± 15.7 ml/min/1.73 m2, T0: 74.6 ± 28.2 ml/min/1.73 m2, p < 0.0001). Endocapillary hypercellularity (E), and glomerular segmental sclerosis (S) were not associated with any clinical outcome parameter. In the analyzed cohort, patients with glomerular crescents (C1/2 scores) in their biopsies were more likely to develop ESRD during the 3-year trial phase, but this trend was only significant in patients under supportive care.
Conclusions: This secondary analysis of STOP-IgAN biopsies indicates that M1, T1/2 and C1/2 scores associate with worse renal outcomes.
Keywords: IgA nephropathy; IgAN; MEST-C; Oxford classification; STOP-IgAN.
Conflict of interest statement
Ethics approval and consent to participate
The original study protocol of STOP-IgAN was amended in 2009 and allowed to retrieve all available original renal biopsies from randomized trial participants. Written informed consent for re-assessment of available kidney biopsies was obtained from all patients included in this secondary substudy. The STOP-IgAN trial as well as the current substudy were approved by the Ethics Committee at the RWTH Aachen University Hospital (reference number 159/07).
Consent for publication
Not applicable.
Competing interests
J. Floege has received consultant honoraria from Omeros, USA and Pharmalink, Sweden, and investigator fees from Anthera Pharmaceuticals Inc., USA. The other authors declare no competing financial interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
