

Clinical course, treatment and outcome of Pneumocystis pneumonia in immunocompromised adults: a retrospective analysis over 17 years
- PMID: 30454031
- PMCID: PMC6245758
- DOI: 10.1186/s13054-018-2221-8
Clinical course, treatment and outcome of Pneumocystis pneumonia in immunocompromised adults: a retrospective analysis over 17 years
Abstract
Background: Despite modern intensive care with standardized strategies against acute respiratory distress syndrome (ARDS), Pneumocystis pneumonia (PcP) remains a life-threatening disease with a high mortality rate. Here, we analyzed a large mixed cohort of immunocompromised patients with PcP, with regard to clinical course and treatment, and aimed at identifying predictors of outcome.
Methods: This was a single-center retrospective analysis in a tertiary care institution across 17 years. Diagnosis of PcP required typical clinical features and microbiological confirmation of Pneumocystis jirovecii. Epidemiological, clinical, laboratory and outcome data were collected from patient records.
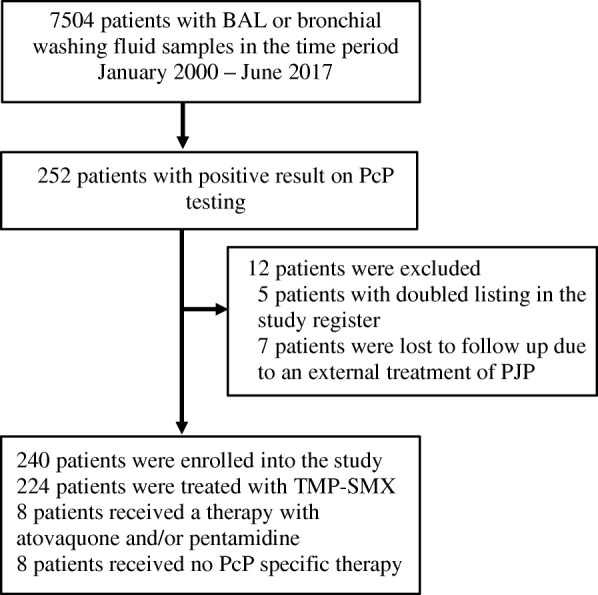
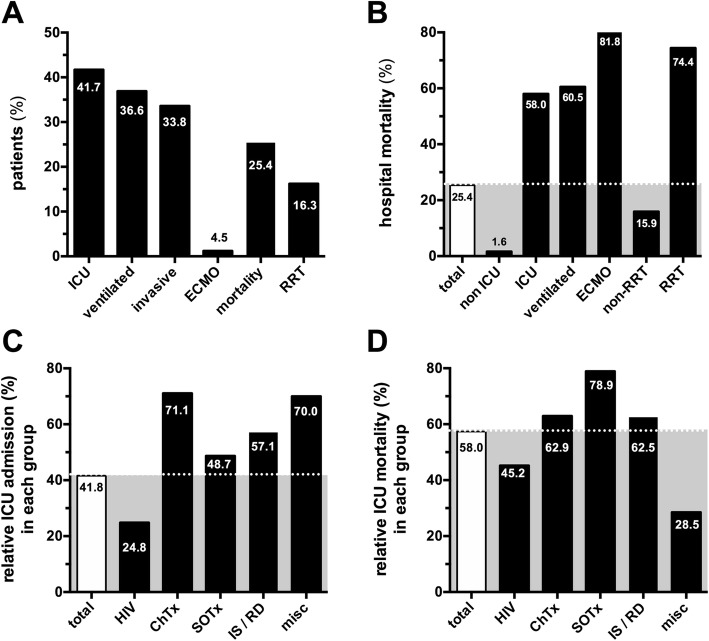
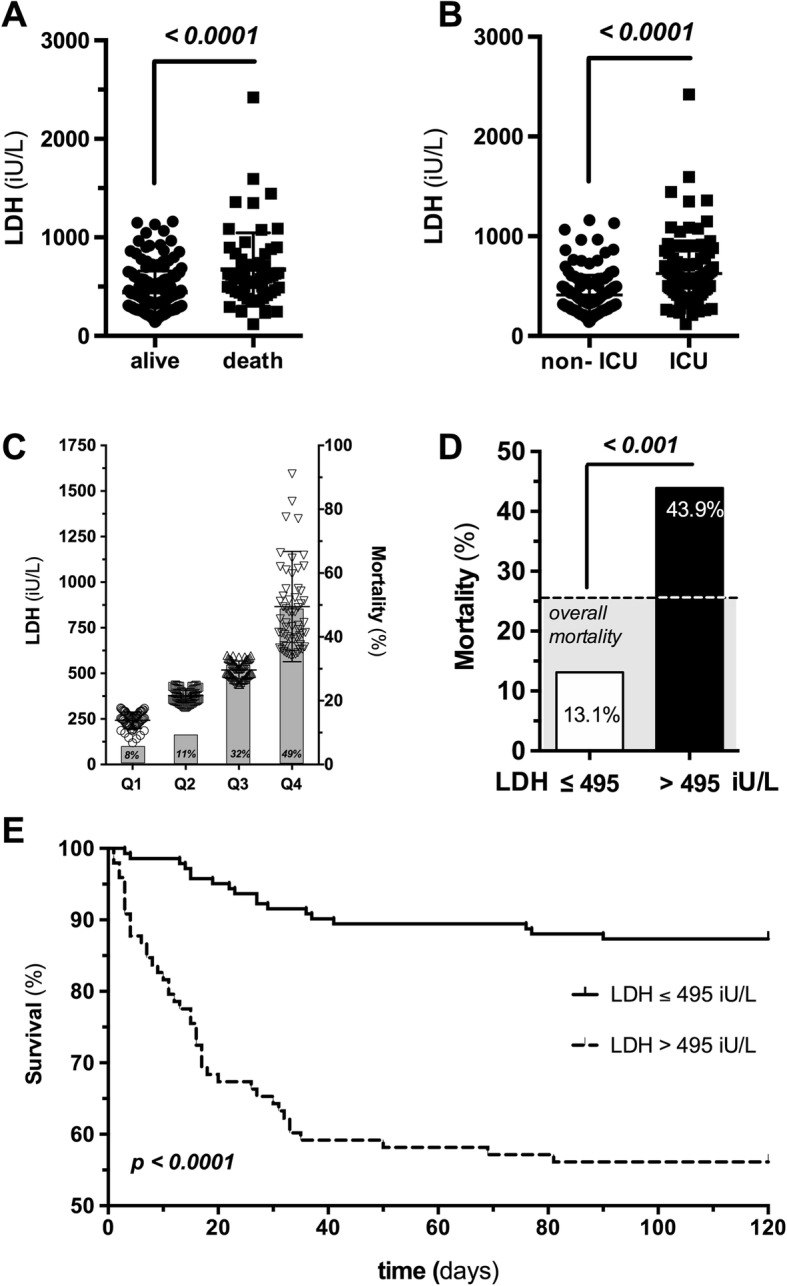
Results: A total of 52,364 specimens from 7504 patients were sent for microbiological assessment (3653 with clinical suspicion of Pneumocystis pneumonia). PcP was confirmed in 240 patients, about half of them HIV positive (52%). The remaining subjects were either solid organ transplant recipients (16.3%) or suffered from malignancy (15.8%) or autoimmune diseases (11.7%). Of note, 95% of patients with PcP were not receiving chemoprophylaxis. Overall in-hospital mortality was 25.4%, increasing to 58% if ICU admission was required. Multivariable regression identified lactate dehydrogenase (LDH) as predictor of in-hospital mortality (adjusted OR 1.17 (95% CI 1.09-1.27), p < 0.0001). Mortality in LDH quartiles increased from 8% to 49%, and a cutoff value of 495 U/L predicted mortality with sensitivity and specificity of 70%. With regard to treatment, 40% of patients received trimethoprim-sulfamethoxazole at doses that were lower than recommended, and these patients had a higher mortality risk (HR 1.80 (95% CI 1.10-3.44), p = 0.02).
Conclusions: PcP remains a life-threatening disease among immunocompromised patients. About half of patients with PcP do not have HIV infection. Initial LDH values might serve as a stratifying tool to identify those patients at high risk of death among patients with HIV and without HIV infection.
Keywords: HIV; LDH; Lactate dehydrogenase; Mortality; Transplantation.
Conflict of interest statement
Ethics approval and consent to participate
Written informed consent was waived by the local ethics committee at Hannover Medical School due to the anonymized retrospective nature of the analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Vanek J, Jirovec O. Parasitic pneumonia. Interstitial plasma cell pneumonia of premature, caused by Pneumocystis carinii. Zentralbl Bakteriol Parasitenkd Infektionskr Hyg. 1952;158:120–127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
