

Trajectory of Excess Medical Expenditures 10 Years Before and After Diabetes Diagnosis Among U.S. Adults Aged 25-64 Years, 2001-2013
- PMID: 30455325
- PMCID: PMC6393199
- DOI: 10.2337/dc17-2683
Trajectory of Excess Medical Expenditures 10 Years Before and After Diabetes Diagnosis Among U.S. Adults Aged 25-64 Years, 2001-2013
Abstract
Objective: We assessed the excess medical expenditures for adults newly diagnosed with diabetes, for up to 10 years before and after diabetes diagnosis.
Research design and methods: Using the 2001-2013 MarketScan data, we identified people with newly diagnosed diabetes among adults aged 25-64 years (diabetes cohort) and matched them with people who did not have diagnosed diabetes (control cohort) using 1:1 propensity score matching. We followed these two cohorts up to ±10 years from the index date, with annual matched cohort sizes ranging from 3,922 to 39,726 individuals. We estimated the yearly and cumulative excess medical expenditures of the diabetes cohorts before and after the diagnosis of diabetes.
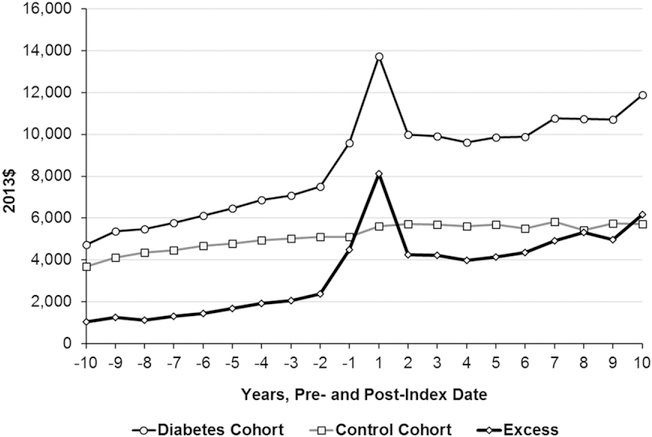
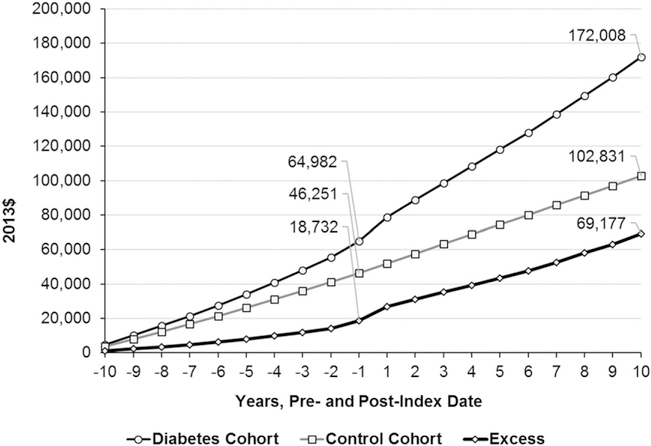
Results: The per capita annual total excess medical expenditure for the diabetes cohort was higher for the entire 10 years prior to their index date, ranging between $1,043 in year -10 and $4,492 in year -1. Excess expenditure spiked in year 1 ($8,109), declined in year 2, and then increased steadily, ranging from $4,261 to $6,162 in years 2-10. The cumulative excess expenditure for the diabetes cohort during the entire 20 years of follow-up was $69,177 ($18,732 before and $50,445 after diagnosis).
Conclusions: People diagnosed with diabetes had higher medical expenditures compared with their counterparts, not only after diagnosis but also up to 10 years prior to diagnosis. Managing risk factors for type 2 diabetes and cardiovascular disease before diagnosis, and for diabetes-related complications after diagnosis, could alleviate medical expenditure in people with diabetes.
© 2018 by the American Diabetes Association.
Conflict of interest statement
Figures
References
-
- Alva ML, Gray A, Mihaylova B, Leal J, Holman RR. The impact of diabetes-related complications on healthcare costs: new results from the UKPDS (UKPDS 84). Diabet Med 2015;32:459–466 - PubMed
-
- Zhuo X, Zhang P, Hoerger TJ. Lifetime direct medical costs of treating type 2 diabetes and diabetic complications. Am J Prev Med 2013; 45:253–261 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
