

Next generation flow for minimally-invasive blood characterization of MGUS and multiple myeloma at diagnosis based on circulating tumor plasma cells (CTPC)
- PMID: 30455467
- PMCID: PMC6242818
- DOI: 10.1038/s41408-018-0153-9
Next generation flow for minimally-invasive blood characterization of MGUS and multiple myeloma at diagnosis based on circulating tumor plasma cells (CTPC)
Abstract
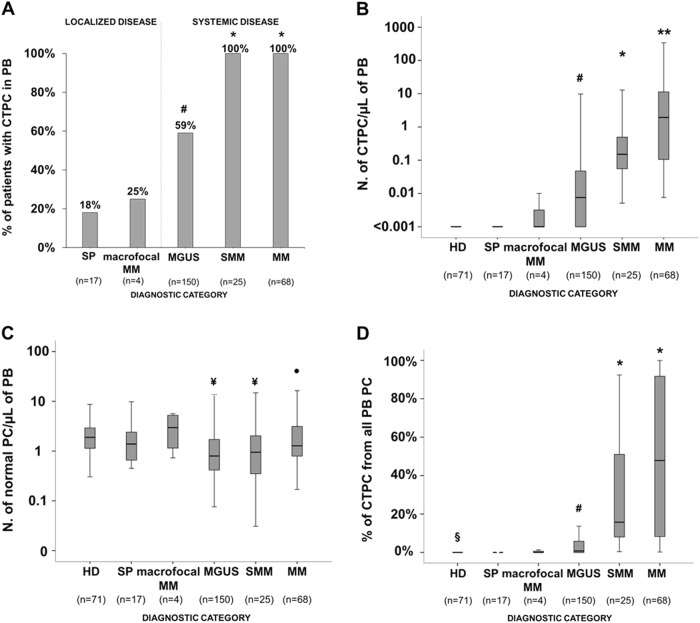
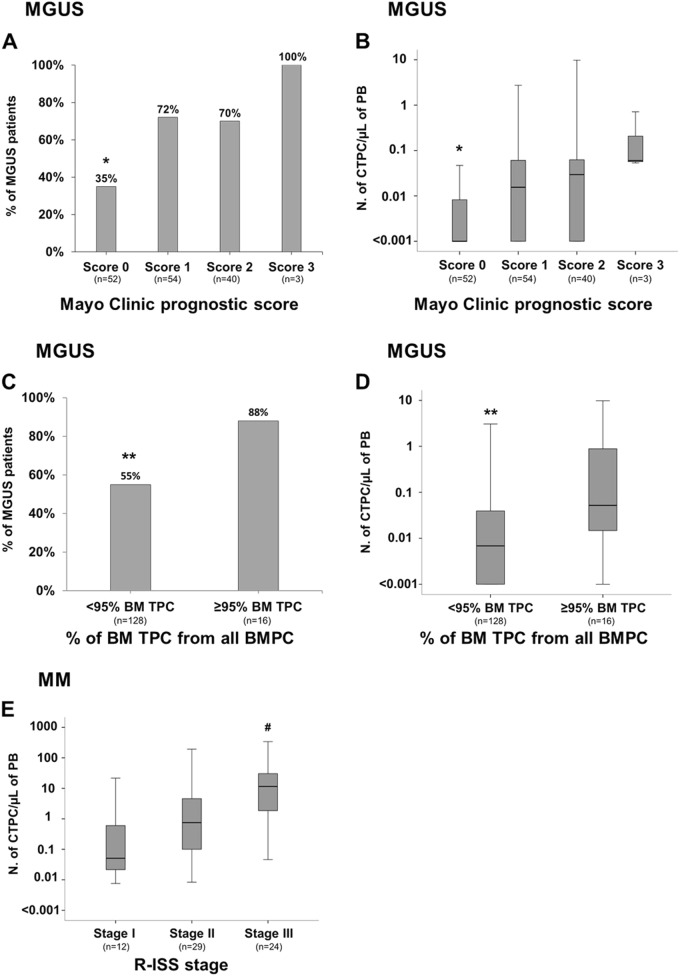
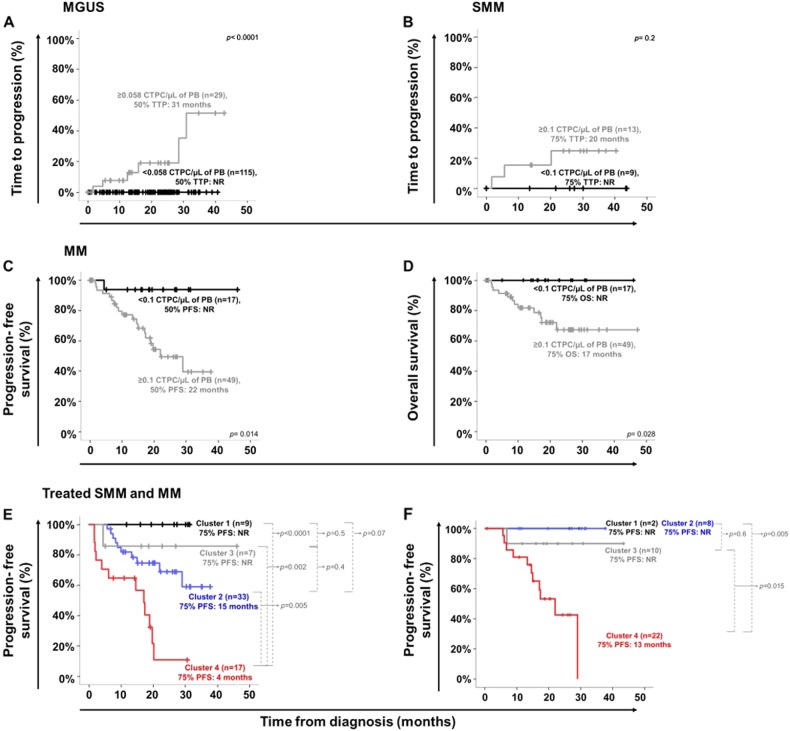
Here, we investigated for the first time the frequency and number of circulating tumor plasma cells (CTPC) in peripheral blood (PB) of newly diagnosed patients with localized and systemic plasma cell neoplasms (PCN) using next-generation flow cytometry (NGF) and correlated our findings with the distinct diagnostic and prognostic categories of the disease. Overall, 508 samples from 264 newly diagnosed PCN patients, were studied. CTPC were detected in PB of all active multiple myeloma (MM; 100%), and smoldering MM (SMM) patients (100%), and in more than half (59%) monoclonal gammopathy of undetermined significance (MGUS) cases (p <0.0001); in contrast, CTPC were present in a small fraction of solitary plasmacytoma patients (18%). Higher numbers of CTPC in PB were associated with higher levels of BM infiltration and more adverse prognostic features, together with shorter time to progression from MGUS to MM (p <0.0001) and a shorter survival in MM patients with active disease requiring treatment (p ≤ 0.03). In summary, the presence of CTPC in PB as assessed by NGF at diagnosis, emerges as a hallmark of disseminated PCN, higher numbers of PB CTPC being strongly associated with a malignant disease behavior and a poorer outcome of both MGUS and MM.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- McKenna R. W. et al. In World Health Organization Calssification of Tumours of Haematopoietic and Lymphoid Tissue IARC. pp. 200–208 (Lyon, 2008)
