

Case Reports
doi: 10.1002/ccr3.1758.
eCollection 2018 Nov.
Splinting and mechanical disruption of the mitral valve apparatus by an endocardial left ventricular lead while delivering cardiac resynchronization therapy
Affiliations
- PMID: 30455895
- PMCID: PMC6230603
- DOI: 10.1002/ccr3.1758
Item in Clipboard
Case Reports
Splinting and mechanical disruption of the mitral valve apparatus by an endocardial left ventricular lead while delivering cardiac resynchronization therapy
Clin Case Rep.
.
Abstract
Splinting and mechanical disruption of the mitral valve apparatus is an important limitation of an endocardial left ventricular (LV) pacing lead. Further, long-term data are required before this approach is more widely adopted.
Keywords: cardiac resynchronization therapy; endocardial LV; mitral regurgitation; mitral valve.
Figures

Postprocedural posteroanterior (PA ) X‐ray. LV endocardial lead placed into the basal posterolateral wall. RA lead, RV pace‐sense and separate, defibrillator lead in conventional positions
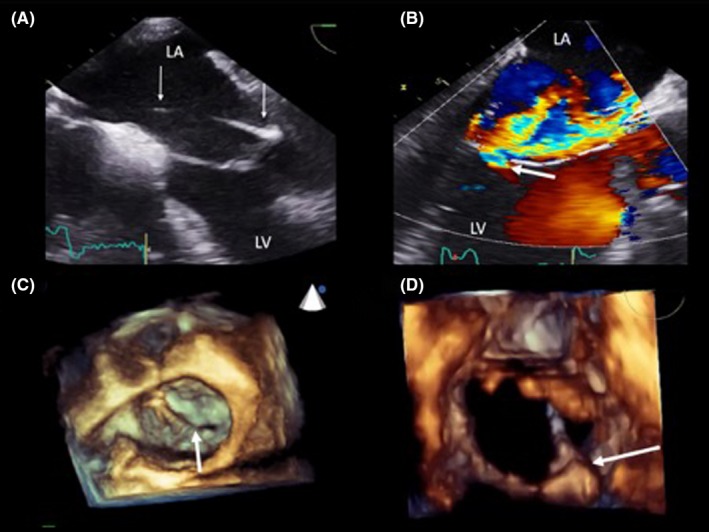
Trans‐esophageal echocardiogram (TEE ). The LV lead is crossing the LA toward the posterior mitral valve leaflet at 0 degree (panel A). There is significant valvular regurgitation depicted by the white arrow at 120 degrees (panel B). Three‐dimensional reconstruction shows an en‐face view of the mitral valve with the white arrow demonstrating the endocardial LV lead preventing complete apposition of mitral valve leaflets at the P2/A2 scallops (panel C). The lead penetrates the mitral valve orifice at P2 (panel D)

Trans‐esophageal echocardiography (TEE). The LV lead is traversing the interatrial septum inferiorly en route to the LA , prior to extraction at 90 degrees (panel A). A residual left to right shunt demonstrated using color Doppler after removal of the lead at 90 degrees (panel B). There is residual mitral regurgitation but significantly less than prior to removal (panel C). Three‐dimensional en‐face reconstruction of the mitral valve apparatus showing a residual deficit at the P2 scallop (panel D)

PA X‐Ray with original CRTD in situ and displaced right atrial lead (panel A). Selective coronary sinus venogram showing a large posterolateral vein with several tributaries and a middle cardiac vein along the inferior surface of the heart (panel B). PA projection X‐Ray of the final, new LV lead position (panel C). The cardiac silhouette is significantly larger; splaying of the carina suggests enlarged atria as a consequence of the severe mitral regurgitation compared with panel A, one year earlier. The quadripolar LV lead was reimplanted into a different distal sub‐branch of the posterolateral vein compared with the original implant.
References
-
- Domenichini G, Diab I, Campbell NG, et al. A highly effective technique for transseptal endocardial left ventricular lead placement for delivery of cardiac resynchronization therapy. Heart Rhythm. 2015;12:943‐949. - PubMed
-
- Derval N, Steendijk P, Gula LJ, et al. Optimizing hemodynamics in heart failure patients by systematic screening of left ventricular pacing sites: the lateral left ventricular wall and the coronary sinus are rarely the best sites. J Am Coll Cardiol. 2010;55:566‐575. - PubMed
-
- Spragg DD, Dong J, Fetics BJ, et al. Optimal left ventricular endocardial pacing sites for cardiac resynchronization therapy in patients with ischemic cardiomyopathy. J Am Coll Cardiol. 2010;56:774‐781. - PubMed
-
- Shetty AK, Sohal M, Chen Z, et al. A comparison of left ventricular endocardial, multisite, and multipolar epicardial cardiac resynchronization: an acute haemodynamic and electroanatomical study. Europace. 2014;16:873‐879. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
