

Revision Surgery for Vestibular Schwannomas
- PMID: 30456020
- PMCID: PMC6239869
- DOI: 10.1055/s-0038-1635256
Revision Surgery for Vestibular Schwannomas
Abstract
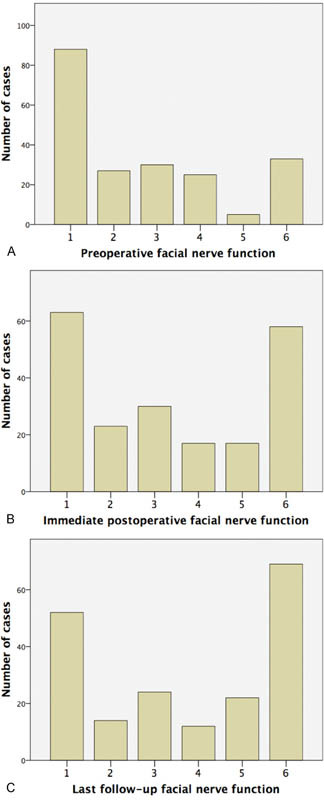
Objectives To describe clinical outcomes of patients undergoing revision surgery for vestibular schwannomas. Design Retrospective case series. Setting Tertiary private neurotologic practice. Participants Patients who underwent revision surgeries for recurrent/residual vestibular schwannomas between 1985 and 2015. Main Outcome Measures Degree of resection, facial nerve function, cerebrospinal fluid (CSF) leak. Results A total of 234 patients underwent 250 revision surgeries for recurrent/residual vestibular schwannomas. Of these, 86 carried a diagnosis of neurofibromatosis type 2 (NF2). The mean number of prior surgeries was 1.26, and 197 (85%) prior surgeries had been performed elsewhere. The average age at surgery was 43. The most common approach employed at the time of revision surgery was translabyrinthine (87%), followed by transcochlear (6%), middle fossa (5%), and retrosigmoid (2%). Gross total resection was achieved in 212 revision surgeries (85%). Preoperative House-Brackmann facial nerve function was similar in non-NF2 and NF2 groups (mean: 2.7). Mean postoperative facial nerve function at last follow-up was 3.8 in the non-NF2 group and 3.9 in the NF2 group. History of radiation and the extent of resection were not associated with differences in facial nerve function preoperatively or postoperatively. CSF leaks occurred after 21 surgeries (8%), and six (2%) patients required reoperation. Conclusions This is the largest series of revision surgery for vestibular schwannomas to date. Our preferred approach is the translabyrinthine craniotomy, which can be readily modified to include the transcochlear approach for improved access. CSF leak rate slightly exceeds that of primary surgery, and gross total resection is achievable in the vast majority of patients.
Keywords: acoustic neuroma; microsurgery; middle fossa approach; retrosigmoid approach; translabyrinthine approach; vestibular schwannoma.
Figures
References
-
- Stangerup S E, Caye-Thomasen P, Tos M, Thomsen J. The natural history of vestibular schwannoma. Otol Neurotol. 2006;27(04):547–552. - PubMed
-
- Yoshimoto Y. Systematic review of the natural history of vestibular schwannoma. J Neurosurg. 2005;103(01):59–63. - PubMed
-
- Rutherford S A, King A T. Vestibular schwannoma management: what is the ‘best’ option? Br J Neurosurg. 2005;19(04):309–316. - PubMed
-
- Lanman T H, Brackmann D E, Hitselberger W E, Subin B. Report of 190 consecutive cases of large acoustic tumors (vestibular schwannoma) removed via the translabyrinthine approach. J Neurosurg. 1999;90(04):617–623. - PubMed
-
- Friedman R A, Kesser B, Brackmann D E, Fisher L M, Slattery W H, Hitselberger W E. Long-term hearing preservation after middle fossa removal of vestibular schwannoma. Otolaryngol Head Neck Surg. 2003;129(06):660–665. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
