

Review of diffuse cortical injury on diffusion-weighted imaging in acutely encephalopathic patients with an acronym: "CRUMPLED"
- PMID: 30456218
- PMCID: PMC6231053
- DOI: 10.1016/j.ejro.2018.10.004
Review of diffuse cortical injury on diffusion-weighted imaging in acutely encephalopathic patients with an acronym: "CRUMPLED"
Abstract
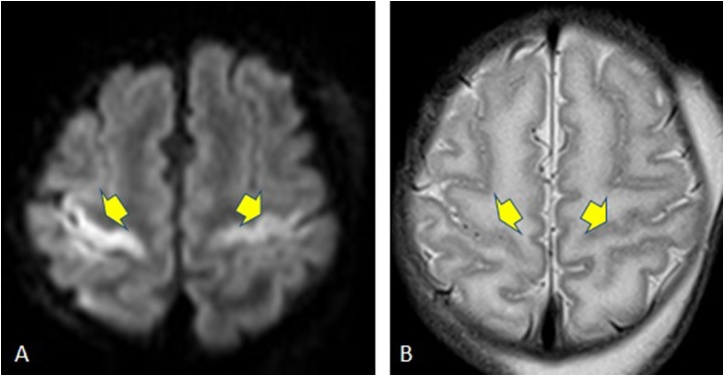
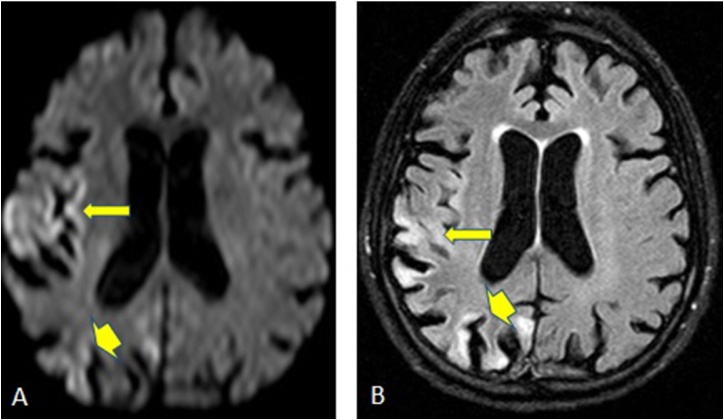
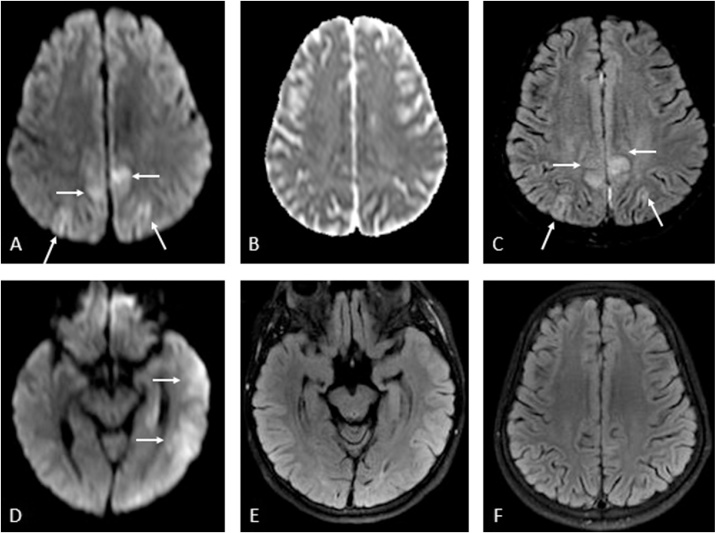
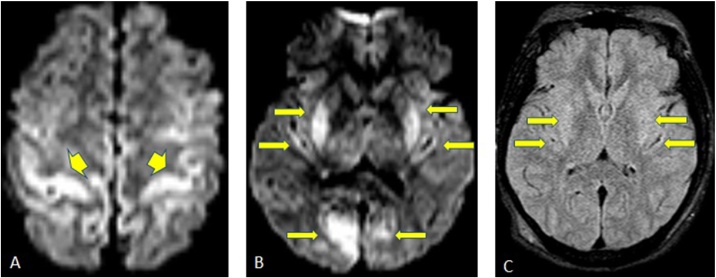
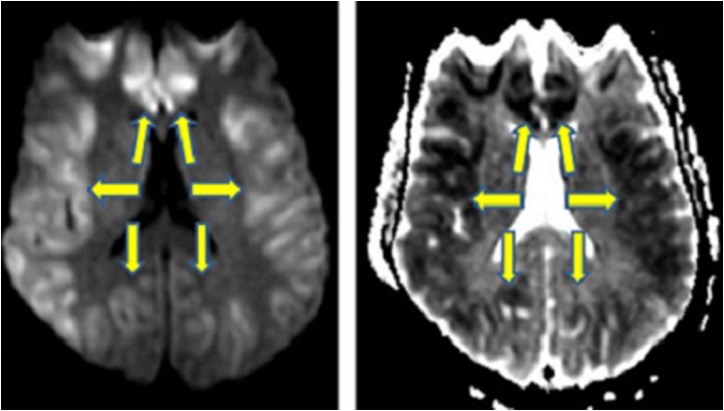
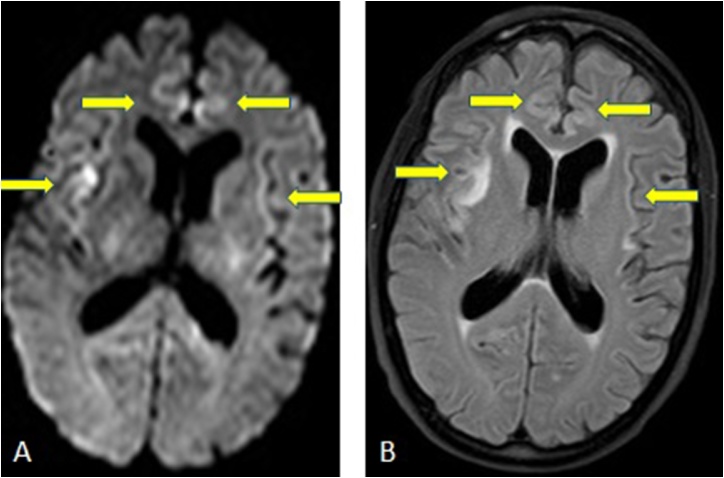
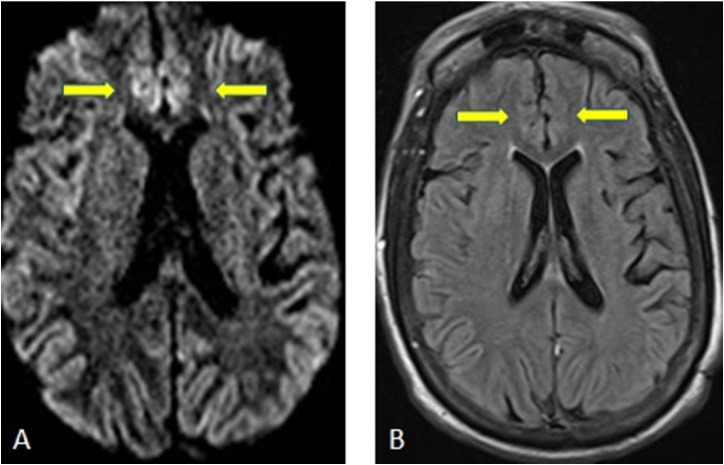
Purpose: Acute encephalopathic syndromes can present a diagnostic challenge due to the wide range of possible etiologies, which also can have vastly different outcomes. The presence of diffuse cortical injury (DCI) on diffusion-weighted imaging (DWI) can help narrow the differential diagnosis. The aim of this review is to categorize the range of possible etiologies of DCI into a useful acronym, "CRUMPLED".
Methods: A review of the PACS system was completed to find a characteristic example of patients with DCI on DWI from different etiologies. The diagnosis was confirmed for each example via a subsequent review of the electronic medical record used to assess for data such as biopsy results, laboratory values, and clinical correlation. The electronic exhibit intends to demonstrate several sample cases of each letter within the acronym, and to demonstrate which types of DCI are potentially reversible or irreversible.
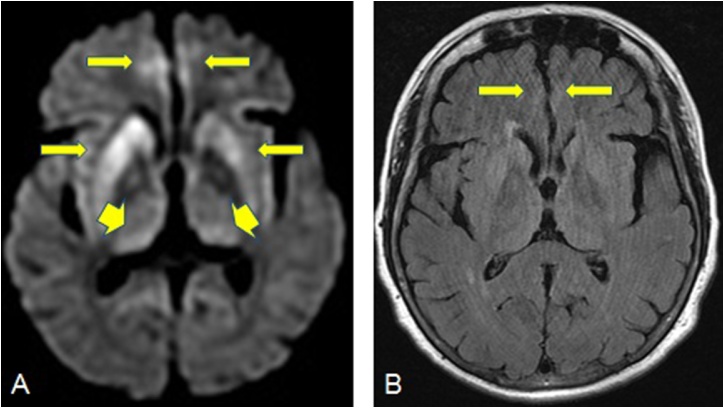
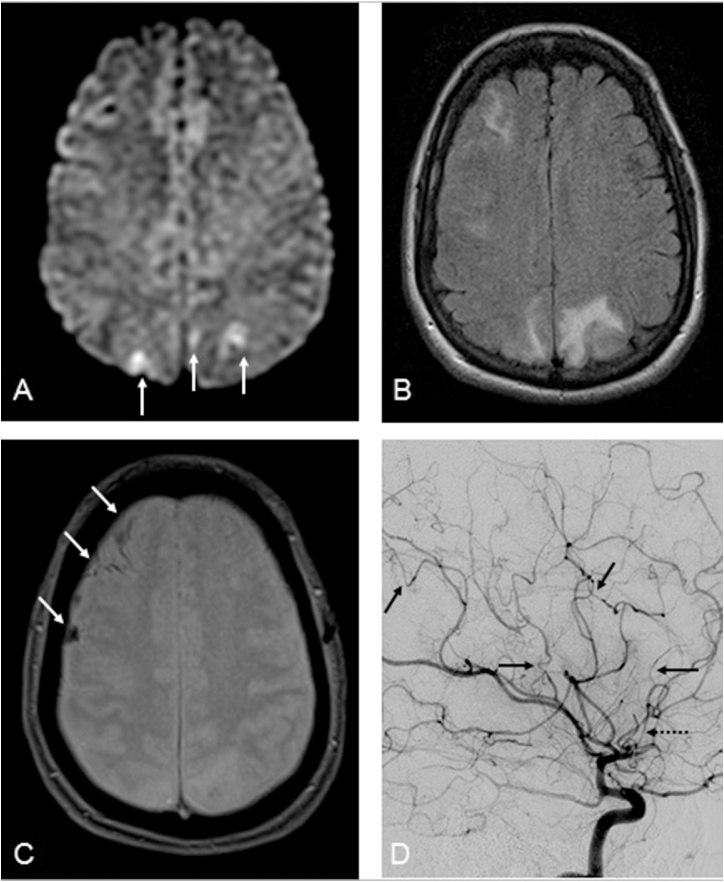
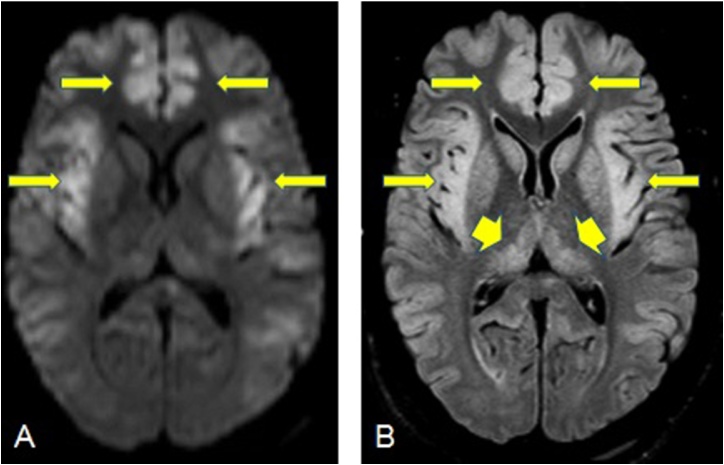
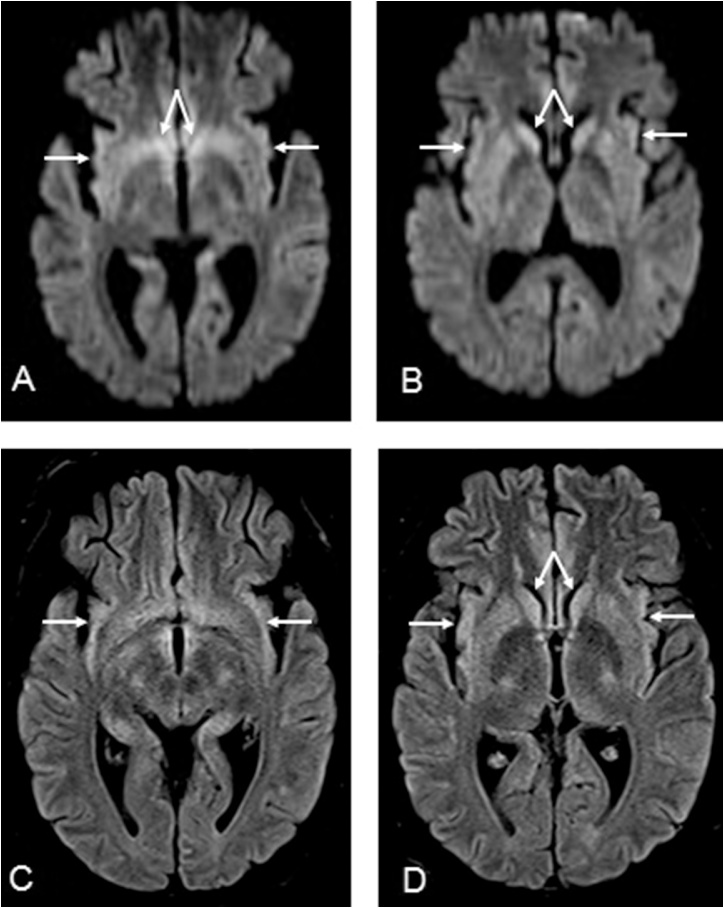
Findings/discussion: The possible etiologies of DCI on DWI can be organized using the acronym "CRUMPLED": 'C' = Creutzfeldt-jakob disease, 'R' = reversible cerebral vasoconstriction syndrome; 'U' = urea cycle disorders (hyperammonemia) and Uremia; 'M' = mitochondrial (cytopathy/encephalopathy); 'P' = prolonged seizure and posterior reversible encephalopathy (PRES); 'L' = laminar necrosis (hypoxic-ischemic encephalopathy) and liver disease (acute hepatic encephalopathy); 'E' = encephalitis (infectious meningoencephalitis); 'D' = diabetes mellitus (hypoglycemia). Other secondary imaging findings (outside of DWI) can be used to help differentiate between the aforementioned etiologies, such as the use of ADC maps, FLAIR imaging, intravenous contrast.
Conclusion: "CRUMPLED" is proposed as a convenient acronym for the categorization of a diverse range of acute etiologies associated with DCI on DWI, arising from varying degrees of cytotoxic edema. These etiologies can range from being potentially reversible (e.g. hyperammonemia or prolonged seizures) to irreversible (e.g. hypoxic-ischemic injury).
Keywords: AHE, Acute Hepatic/Hyperammonemic Encephalopathy; Acute encephalopathy; CJD, Creutzfeldt-Jakob disease; DCI, Diffuse cortical injury; DWI; Diffuse cortical injury; MELAS, mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes; PRES, Posterior reversible encephalopathy syndrome; RCVS, Reversible cerebral vasoconstriction syndrome; UCD, Urea cycle disorders.
Figures
Similar articles
-
"CHOICES": An acronym to aid in delineating potential causes of non-metabolic, non-infectious acute toxic leukoencephalopathy.Eur J Radiol Open. 2019 Jun 28;6:243-257. doi: 10.1016/j.ejro.2019.06.005. eCollection 2019. Eur J Radiol Open. 2019. PMID: 31309133 Free PMC article. Review.
-
Acute hepatic encephalopathy: diffusion-weighted and fluid-attenuated inversion recovery findings, and correlation with plasma ammonia level and clinical outcome.AJNR Am J Neuroradiol. 2010 Sep;31(8):1471-9. doi: 10.3174/ajnr.A2112. Epub 2010 May 6. AJNR Am J Neuroradiol. 2010. PMID: 20448015 Free PMC article.
-
Use of high b value diffusion-weighted magnetic resonance imaging in acute encephalopathy/encephalitis during childhood.Brain Dev. 2018 Feb;40(2):116-125. doi: 10.1016/j.braindev.2017.07.012. Epub 2017 Aug 31. Brain Dev. 2018. PMID: 28838686
-
Concomitant Acute Toxic Leukoencephalopathy and Posterior Reversible Encephalopathy Syndrome.J Neuroimaging. 2018 Sep;28(5):535-541. doi: 10.1111/jon.12526. Epub 2018 May 24. J Neuroimaging. 2018. PMID: 29797465
-
Potentially Reversible and Recognizable Acute Encephalopathic Syndromes: Disease Categorization and MRI Appearances.AJNR Am J Neuroradiol. 2020 Aug;41(8):1328-1338. doi: 10.3174/ajnr.A6634. Epub 2020 Jul 2. AJNR Am J Neuroradiol. 2020. PMID: 32616580 Free PMC article. Review.
Cited by
-
Diffuse Cortical Injury by Hypoglycemia.Intern Med. 2019 Aug 15;58(16):2415. doi: 10.2169/internalmedicine.2623-19. Epub 2019 May 22. Intern Med. 2019. PMID: 31118389 Free PMC article. No abstract available.
-
The split apparent diffusion coefficient sign: A novel magnetic resonance imaging biomarker for cortical pathology with possible implications in autoimmune encephalitis.Neuroradiol J. 2024 Apr;37(2):206-213. doi: 10.1177/19714009231224416. Epub 2023 Dec 26. Neuroradiol J. 2024. PMID: 38146643 Free PMC article.
-
Challenges for biophysical modeling of microstructure.J Neurosci Methods. 2020 Oct 1;344:108861. doi: 10.1016/j.jneumeth.2020.108861. Epub 2020 Jul 18. J Neurosci Methods. 2020. PMID: 32692999 Free PMC article. Review.
-
Peculiarities of stroke-like lesions on MRI.Eur J Radiol Open. 2019 Jan 12;6:60-61. doi: 10.1016/j.ejro.2019.01.001. eCollection 2019. Eur J Radiol Open. 2019. PMID: 30671500 Free PMC article. No abstract available.
-
Antiseizure medications for post-stroke epilepsy: A real-world prospective cohort study.Brain Behav. 2021 Sep;11(9):e2330. doi: 10.1002/brb3.2330. Epub 2021 Aug 22. Brain Behav. 2021. PMID: 34423590 Free PMC article.
References
-
- Young G.S., Geschwind M.D., Fischbein N.J., Martindale J.L., Henry R.G., Liu S., Lu Y., Wong S., Liu H., Miller B.L., Dillon W.P. Diffusion-weighted and fluid-attenuated inversion recovery imaging in Creutzfeldt-Jakob disease: high sensitivity and specificity for diagnosis. AJNR Am. J. Neuroradiol. 2005;26:1551–1562. - PMC - PubMed
-
- Malhotra K., Liebeskind D.S. Imaging of MELAS. Curr. Pain Headache Rep. 2016;20:54. - PubMed
LinkOut - more resources
Full Text Sources
