

Adrenal crisis presented as acute onset of hypercalcemia and hyponatremia triggered by acute pyelonephritis in a patient with partial hypopituitarism and pre-dialysis chronic kidney disease
- PMID: 30456557
- PMCID: PMC6450993
- DOI: 10.1007/s13730-018-0371-9
Adrenal crisis presented as acute onset of hypercalcemia and hyponatremia triggered by acute pyelonephritis in a patient with partial hypopituitarism and pre-dialysis chronic kidney disease
Abstract
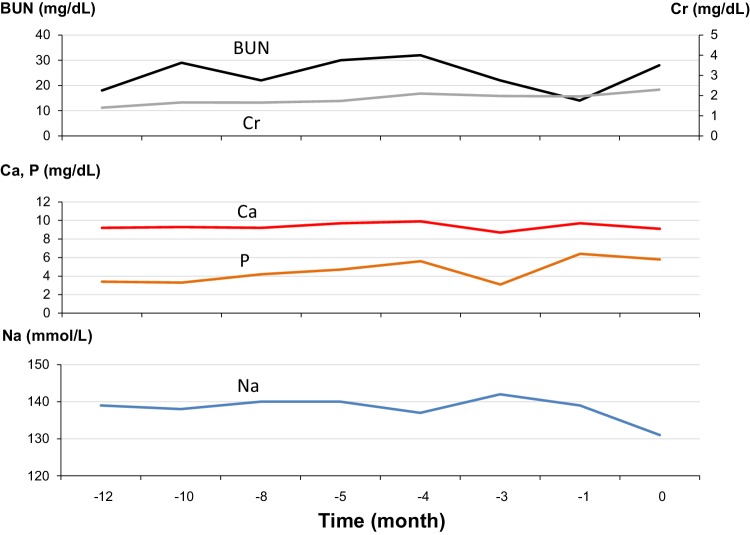
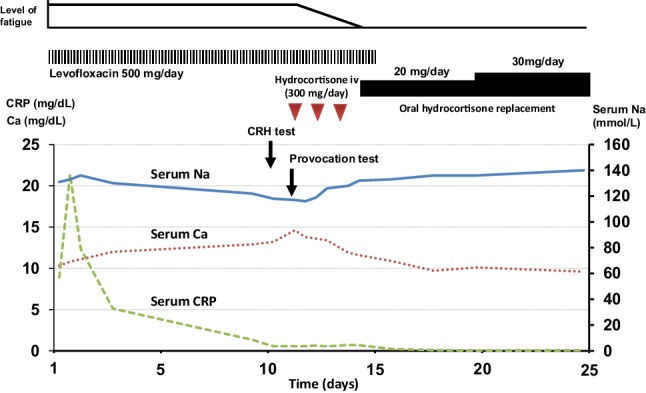
A 57-year-old woman with pre-dialysis chronic kidney disease (CKD) was hospitalized because of fever and fatigue. On admission, increased inflammatory response and pyuria with bacteriuria were observed. Pyelonephritis was successfully treated with antibiotics, whereas her fatigue continued and she developed progressive hypercalcemia and hyponatremia; serum sodium level, 116 mEq/L and corrected serum calcium level, 13.4 mg/dL. Plasma concentrations of adrenocorticotropic hormone and cortisol and serum luteinizing hormone were under the detection level. Although the reaction of other anterior pituitary hormones and the serum antidiuretic hormone (ADH) was preserved, the response of serum luteinizing hormone to administration of luteinizing hormone releasing hormone was impaired. Magnetic resonance imaging showed no structural abnormality in the thalamus, hypothalamus, and pituitary gland. She was diagnosed with adrenal insufficiency caused by partial hypopituitarism in concomitant with pyelonephritis. After starting hydrocortisone replacement, serum levels of sodium and calcium were rapidly normalized. This case highlights the importance of adrenal insufficiency as a differential diagnosis of hypercalcemia in patients with pre-dialysis CKD, especially when hyponatremia was concomitantly observed. Besides, infection should be considered as an important trigger for the development of latent adrenal insufficiency since it could increase the physiological demand of corticosteroid in the body. Also, CKD may enhance the magnitude of hypercalcemia since CKD patients have decreased capacity to increase urinary calcium excretion.
Keywords: Adrenal insufficiency; Chronic kidney disease; Hypercalcemia; Hyponatremia; Partial hypopituitarism.
Conflict of interest statement
Conflict of interest
All the authors declare no competing interest.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
A written informed consent was obtained from the patient included in this case study.
Figures
Similar articles
-
Severe hyponatremia due to hypopituitarism with adrenal insufficiency: report on 28 cases.Eur J Endocrinol. 2003 Jun;148(6):609-17. doi: 10.1530/eje.0.1480609. Eur J Endocrinol. 2003. PMID: 12773132
-
Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) and adrenal insufficiency induced by rathke's cleft cyst: a case report.Endocr J. 2000 Aug;47(4):393-9. doi: 10.1507/endocrj.47.393. Endocr J. 2000. PMID: 11075719
-
Osmoregulation of plasma vasopressin in three cases with adrenal insufficiency of diverse etiologies.Horm Res. 1997;47(1):38-44. doi: 10.1159/000185368. Horm Res. 1997. PMID: 9010716
-
Isolated Adrenocorticotropic Hormone Deficiency Presenting with Severe Hyponatremia and Rhabdomyolysis: A Case Report and Literature Review.Am J Case Rep. 2019 Dec 12;20:1857-1863. doi: 10.12659/AJCR.918427. Am J Case Rep. 2019. PMID: 31827062 Free PMC article. Review.
-
Extrapontine Myelinolysis and Reversible Parkinsonism After Hyponatremia Correction in a Case of Pituitary Adenoma: Hypopituitarism as a Predisposition for Osmotic Demyelination.World Neurosurg. 2018 Oct;118:304-310. doi: 10.1016/j.wneu.2018.07.115. Epub 2018 Jul 25. World Neurosurg. 2018. PMID: 30055367 Review.
Cited by
-
Two-way Road of Kidney and Hypercalcemia: A Narrative Review.Cardiovasc Hematol Disord Drug Targets. 2023;22(4):200-206. doi: 10.2174/1871529X23666221205143041. Cardiovasc Hematol Disord Drug Targets. 2023. PMID: 36475333 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
