

Risk of subsequent fracture after prior fracture among older women
- PMID: 30456571
- PMCID: PMC6332293
- DOI: 10.1007/s00198-018-4732-1
Risk of subsequent fracture after prior fracture among older women
Abstract
Among 377,561 female Medicare beneficiaries who sustained a fracture, 10% had another fracture within 1 year, 18% within 2 years, and 31% within 5 years. Timely management to reduce risk of subsequent fracture is warranted following all nontraumatic fractures, including nonhip nonvertebral fractures, in older women.
Introduction: Prior fracture is a strong predictor of subsequent fracture; however, postfracture treatment rates are low. Quantifying imminent (12-24 month) risk of subsequent fracture in older women may clarify the need for early postfracture management.
Methods: This retrospective cohort study used Medicare administrative claims data. Women ≥ 65 years who sustained a clinical fracture (clinical vertebral and nonvertebral fracture; index date) and were continuously enrolled for 1-year pre-index and ≥ 1-year (≥ 2 or ≥ 5 years for outcomes at those time points) post-index were included. Cumulative incidence of subsequent fracture was calculated from 30 days post-index to 1, 2, and 5 years post-index. For appendicular fractures, only those requiring hospitalization or surgical repair were counted. Death was considered a competing risk.
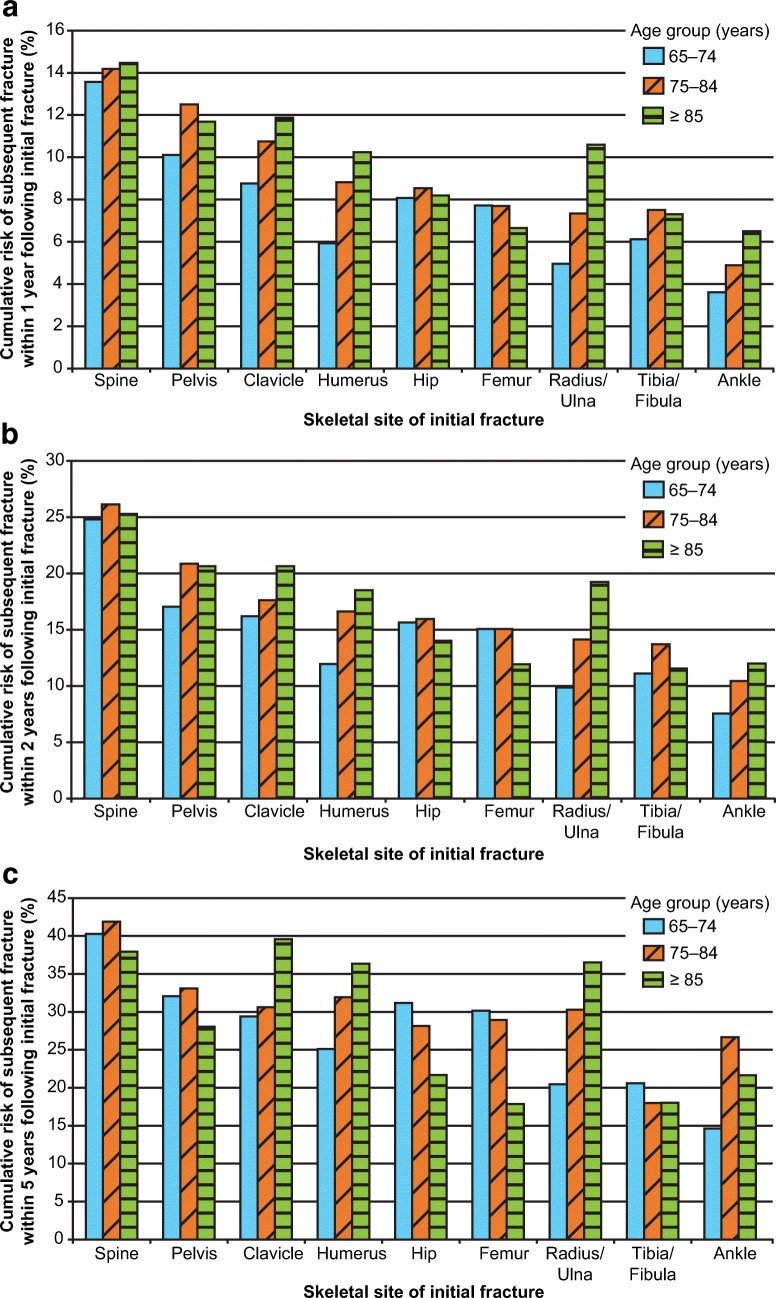
Results: Among 377,561 women (210,621 and 10,969 for 2- and 5-year outcomes), cumulative risk of subsequent fracture was 10%, 18%, and 31% at 1, 2, and 5 years post-index, respectively. Among women age 65-74 years with initial clinical vertebral, hip, pelvis, femur, or clavicle fractures and all women ≥ 75 years regardless of initial fracture site (except ankle and tibia/fibula), 7-14% fractured again within 1 year depending on initial fracture site; risk rose to 15-26% within 2 years and 28-42% within 5 years. Risk of subsequent hip fracture exceeded 3% within 5 years in all women studied, except those < 75 years with an initial tibia/fibula or ankle fracture.
Conclusions: We observed a high and early risk of subsequent fracture following a broad array of initial fractures. Timely management with consideration of pharmacotherapy is warranted in older women following all fracture types evaluated.
Keywords: Epidemiology; Fracture; Fracture risk assessment; Fragility; General population studies; Geriatric; Incidence; Major osteoporotic fracture; Osteoporosis; Postmenopausal; Prediction modeling; Prevalence; Refracture.
Conflict of interest statement
LC and SGD have nothing to disclose. JZ received research support from Amgen Inc. during the conduct of the study. AG and AB are employees of and hold stock in Amgen Inc. DW was an employee of, holds stock in, and has received consulting fees from Amgen Inc. JRC has received research grants and consulting fees from Amgen Inc. and Radius Health.
Figures

References
-
- World Health Organization . WHO scientific group on the assessment of osteoporosis at primary health care level: summary meeting report; 5–7 May 2004. Belgium: Brussels; 2007.
-
- National Committee for Quality Assurance (2014) The state of health care quality 2014. http://store.ncqa.org/index.php/2014-state-of-health-care-quality-report.... Accessed 15 November 2016
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
