

Splanchnic Circulation and Intraabdominal Metabolism in Two Porcine Models of Low Cardiac Output
- PMID: 30456737
- PMCID: PMC6611896
- DOI: 10.1007/s12265-018-9845-6
Splanchnic Circulation and Intraabdominal Metabolism in Two Porcine Models of Low Cardiac Output
Abstract
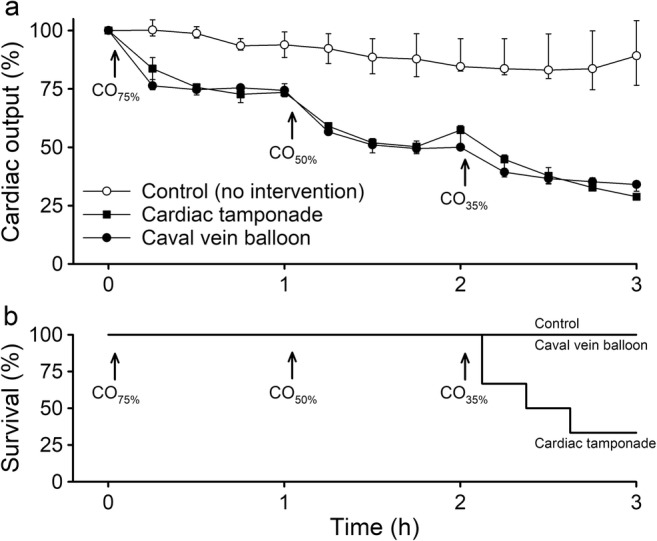
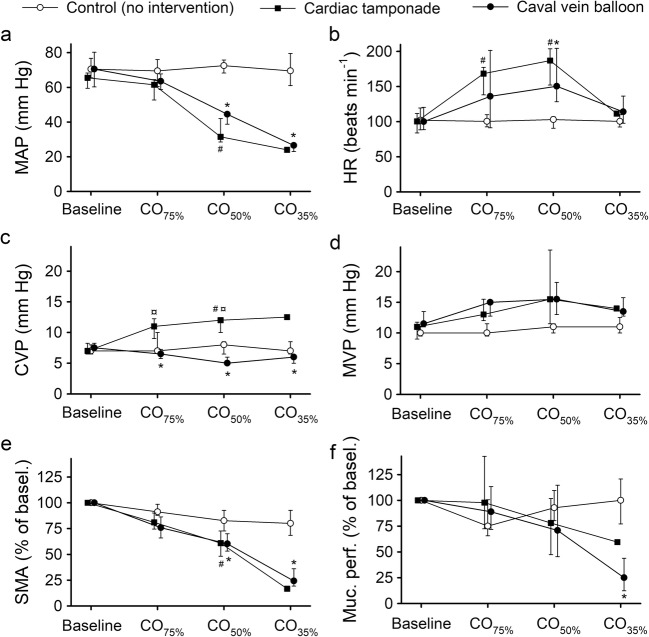
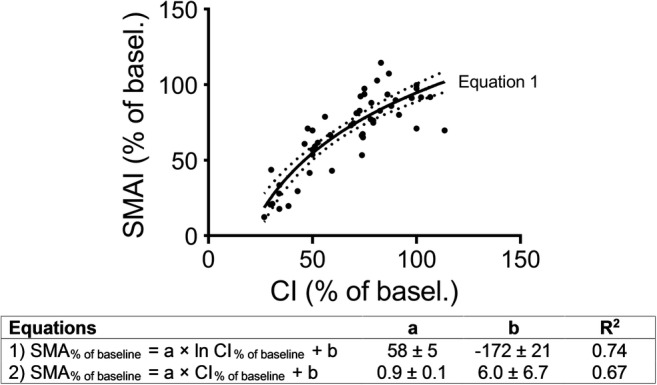
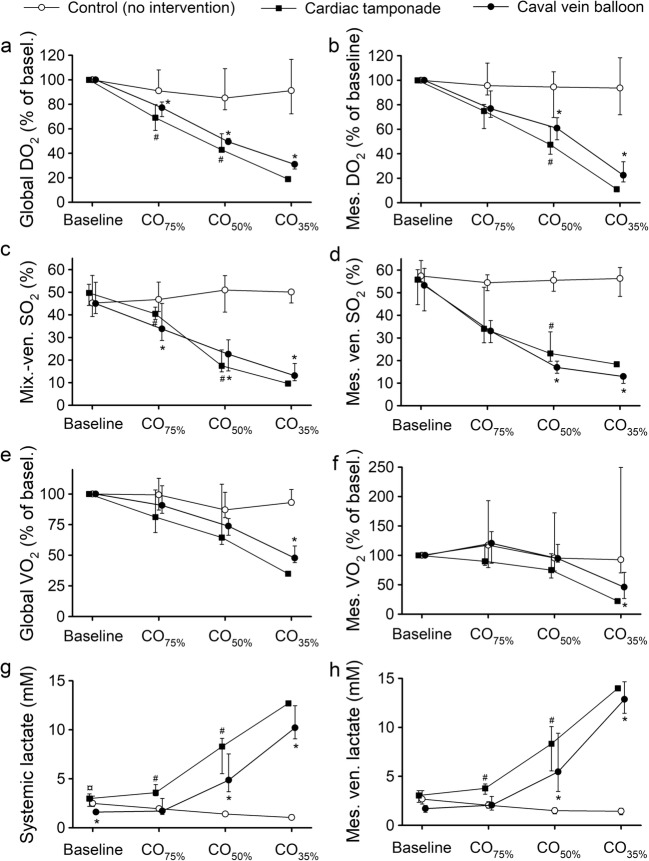
The impact of acute cardiac dysfunction on the gastrointestinal tract was investigated in anesthetized and instrumented pigs by sequential reductions of cardiac output (CO). Using a cardiac tamponade (n = 6) or partial inferior caval vein balloon inflation (n = 6), CO was controllably reduced for 1 h each to 75% (CO75%), 50% (CO50%), and 35% (CO35%) of the baseline value. Cardiac output in controls (n = 6) was not manipulated and maintained. Mean arterial pressure, superior mesenteric arterial blood flow, and intestinal mucosal perfusion started to decrease at CO50% in the intervention groups. The decrease in superior mesenteric arterial blood flow was non-linear and exaggerated at CO35%. Systemic, venous mesenteric, and intraperitoneal lactate concentrations increased in the intervention groups from CO50%. Global and mesenteric oxygen uptake decreased at CO35%. In conclusion, gastrointestinal metabolism became increasingly anaerobic when CO was reduced by 50%. Anaerobic gastrointestinal metabolism in low CO can be detected using intraperitoneal microdialysis.
Keywords: Cardiac dysfunction; Cardiac tamponade; Caval vein balloon; Intraperitoneal microdialysis; Laser Doppler flowmetry; Porcine model.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Chaudhry R, Zaki J, Wegner R, Pednekar G, Tse A, Sheinbaum R, et al. Gastrointestinal complications after cardiac surgery: a nationwide population-based analysis of morbidity and mortality predictors. Journal of Cardiothoracic and Vascular Anesthesia. 2017;31(4):1268–1274. doi: 10.1053/j.jvca.2017.04.013. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
