

Validation of Current Good Manufacturing Practice Compliant Human Pluripotent Stem Cell-Derived Hepatocytes for Cell-Based Therapy
- PMID: 30456803
- PMCID: PMC6344902
- DOI: 10.1002/sctm.18-0084
Validation of Current Good Manufacturing Practice Compliant Human Pluripotent Stem Cell-Derived Hepatocytes for Cell-Based Therapy
Abstract
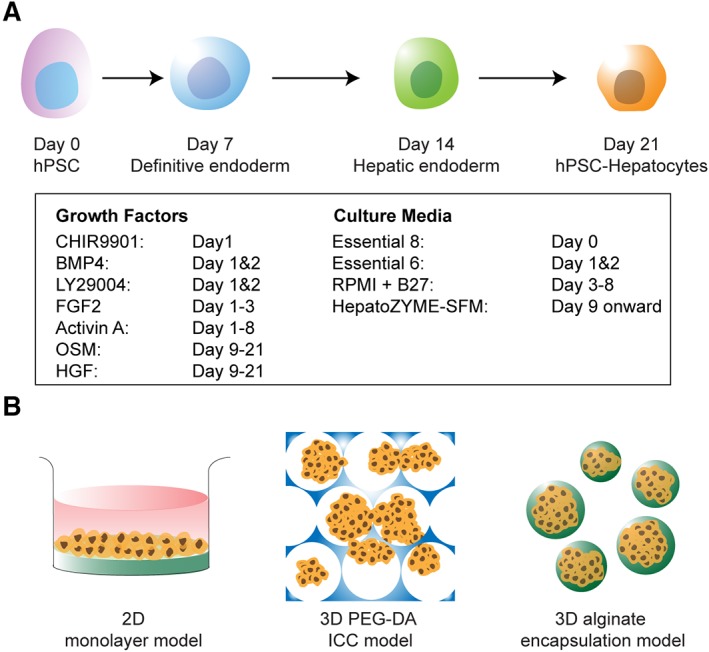
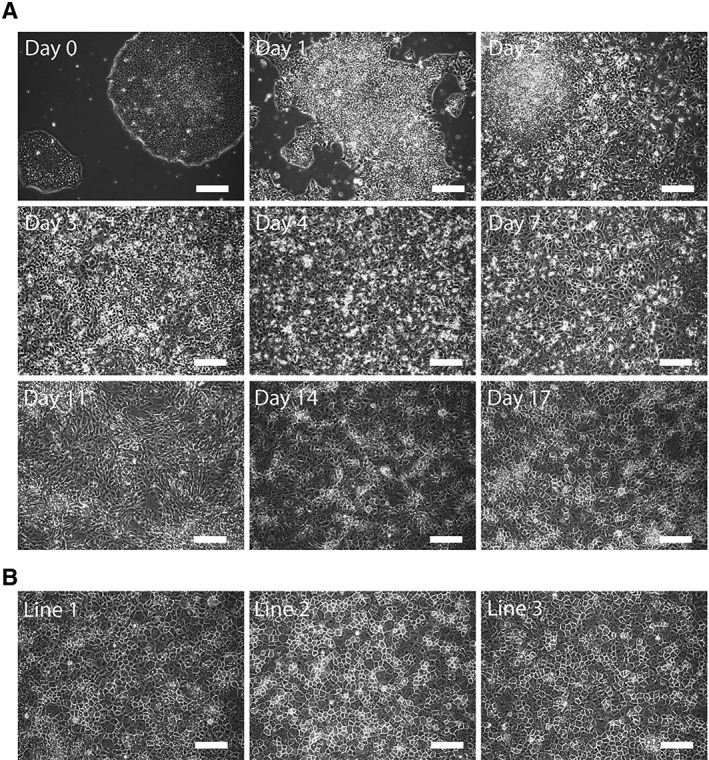
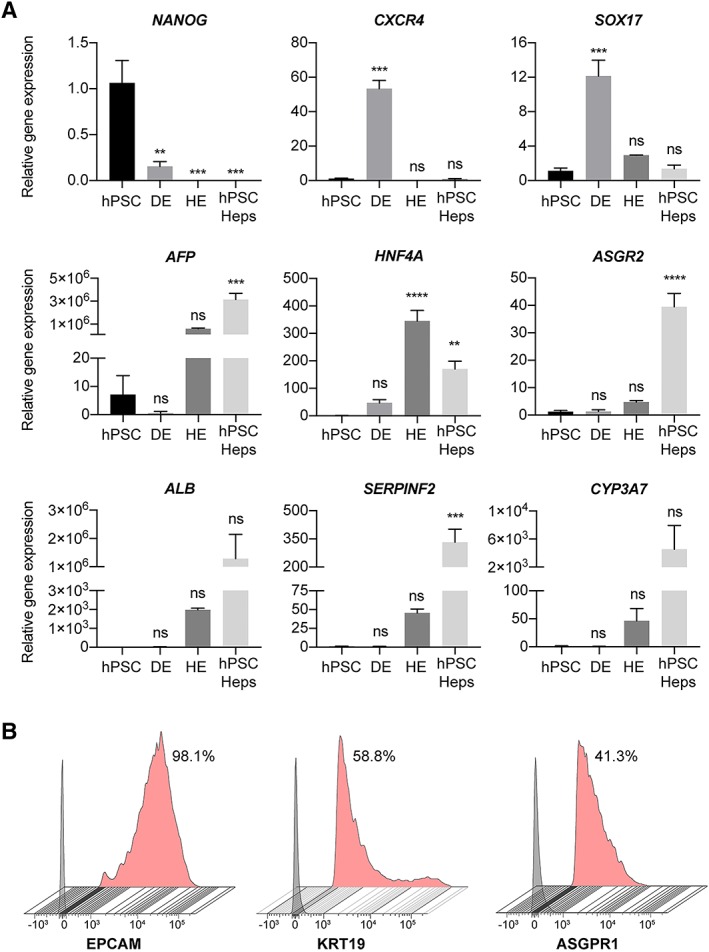
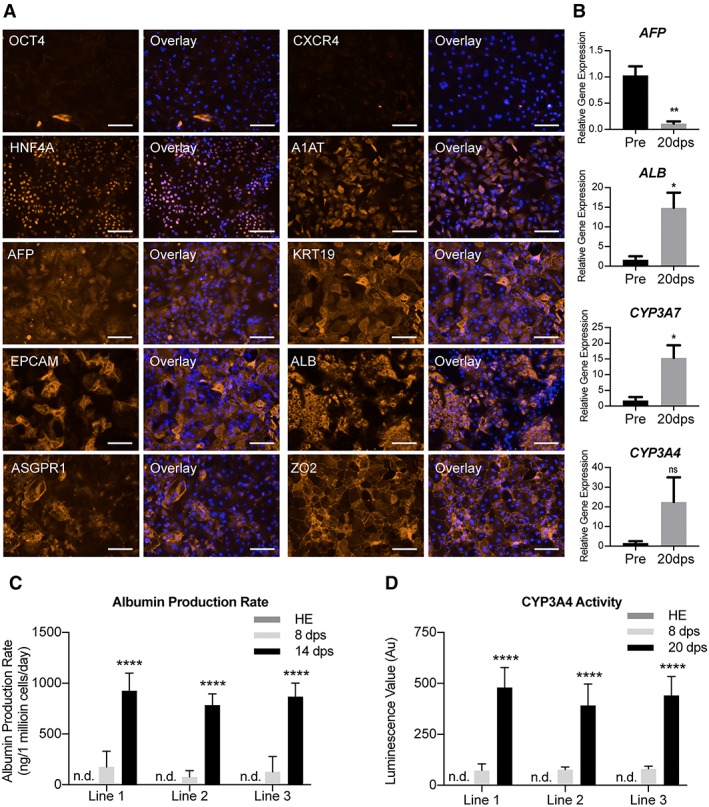
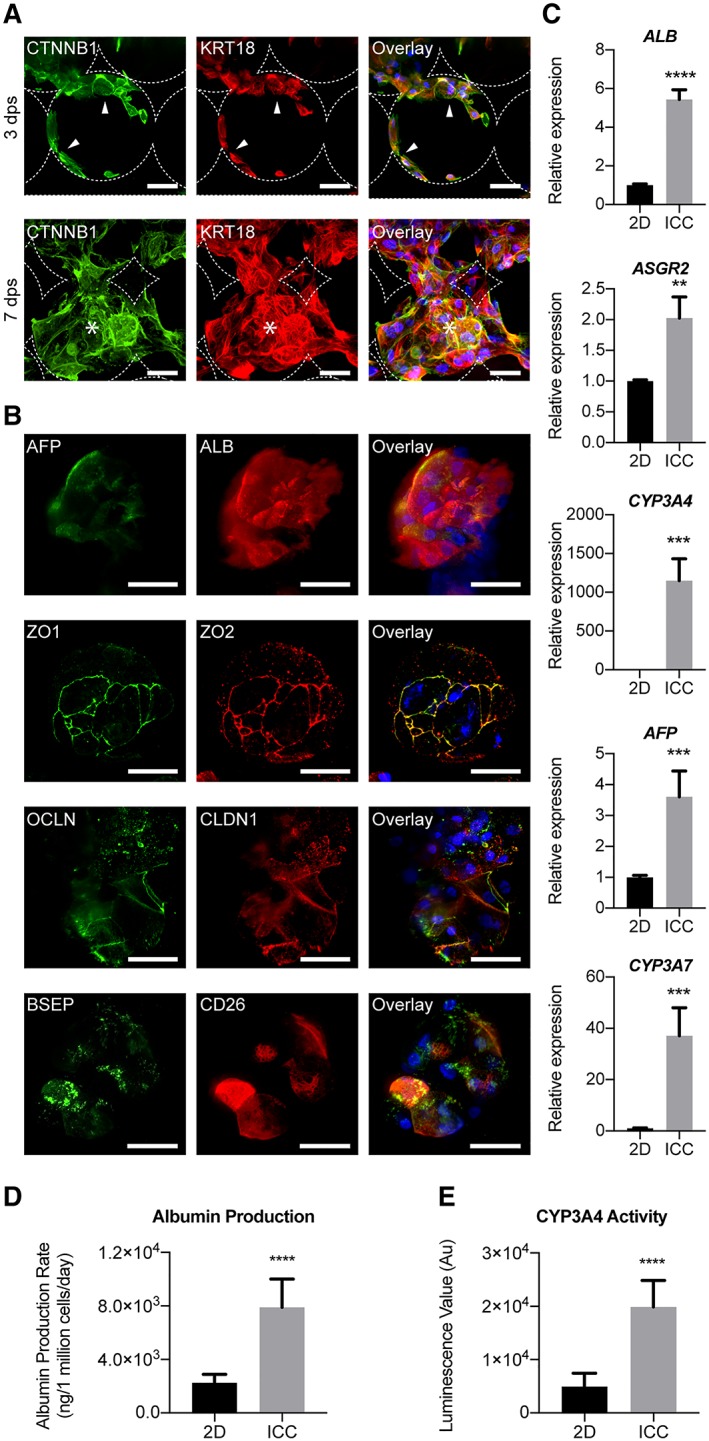
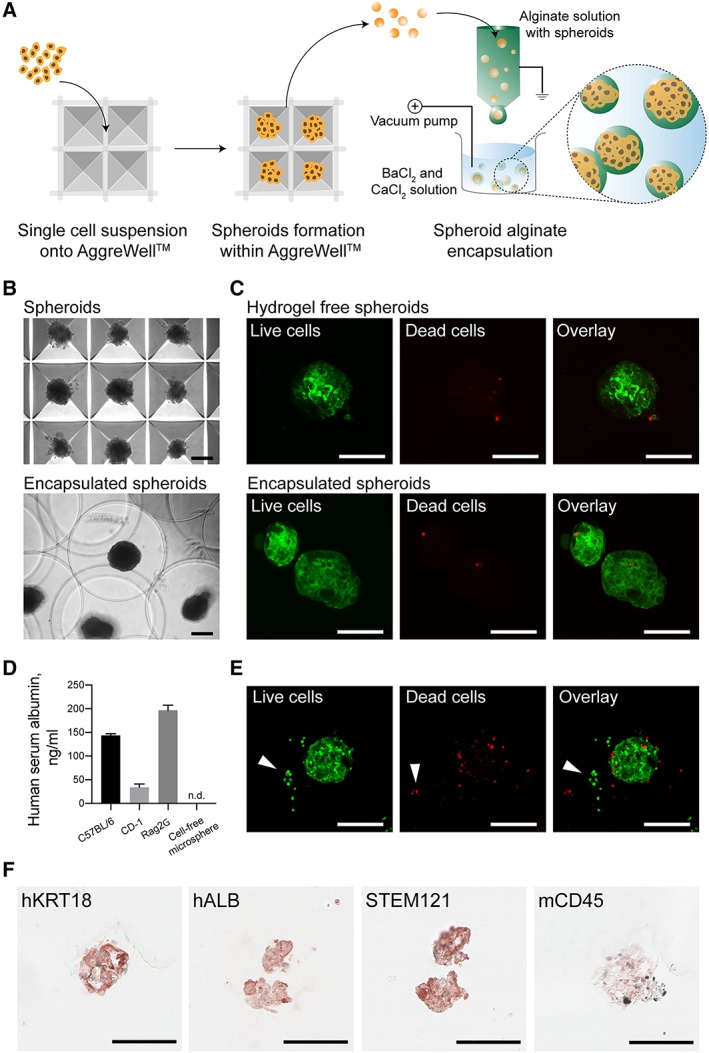
Recent advancements in the production of hepatocytes from human pluripotent stem cells (hPSC-Heps) afford tremendous possibilities for treatment of patients with liver disease. Validated current good manufacturing practice (cGMP) lines are an essential prerequisite for such applications but have only recently been established. Whether such cGMP lines are capable of hepatic differentiation is not known. To address this knowledge gap, we examined the proficiency of three recently derived cGMP lines (two hiPSC and one hESC) to differentiate into hepatocytes and their suitability for therapy. hPSC-Heps generated using a chemically defined four-step hepatic differentiation protocol uniformly demonstrated highly reproducible phenotypes and functionality. Seeding into a 3D poly(ethylene glycol)-diacrylate fabricated inverted colloid crystal scaffold converted these immature progenitors into more advanced hepatic tissue structures. Hepatic constructs could also be successfully encapsulated into the immune-privileged material alginate and remained viable as well as functional upon transplantation into immune competent mice. This is the first report we are aware of demonstrating cGMP-compliant hPSCs can generate cells with advanced hepatic function potentially suitable for future therapeutic applications. Stem Cells Translational Medicine 2019;8:124&14.
Keywords: Bioengineering; Cell transplantation; Cellular therapy; Hepatocyte differentiation; Hepatocytes; Liver therapy; Pluripotent stem cells; cGMP; hESC; iPSC.
© 2018 The Authors. Stem Cells Translational Medicine published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Figures
References
-
- Dhawan A, Mitry RR, Hughes RD et al. Hepatocyte transplantation for inherited factor VII deficiency. Transplantation 2004;78:1812–1814. - PubMed
-
- Meyburg J, Das AM, Hoerster F et al. One liver for four children: First clinical series of liver cell transplantation for severe neonatal urea cycle defects. Transplantation 2009;87:636–641. - PubMed
-
- Beck BB, Habbig S, Dittrich K et al. Liver cell transplantation in severe infantile oxalosisa potential bridging procedure to orthotopic liver transplantation? Nephrol Dial Transplant 2012;27:2984–2989. - PubMed
-
- Iansante V, Mitry RR, Filippi C et al. Human hepatocyte transplantation for liver disease: Current status and future perspectives. Pediatr Res 2017;83:232–240. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
