

IqYmune® is an effective maintenance treatment for multifocal motor neuropathy: A randomised, double-blind, multi-center cross-over non-inferiority study vs Kiovig®-The LIME Study
- PMID: 30456899
- PMCID: PMC6590491
- DOI: 10.1111/jns.12291
IqYmune® is an effective maintenance treatment for multifocal motor neuropathy: A randomised, double-blind, multi-center cross-over non-inferiority study vs Kiovig®-The LIME Study
Abstract
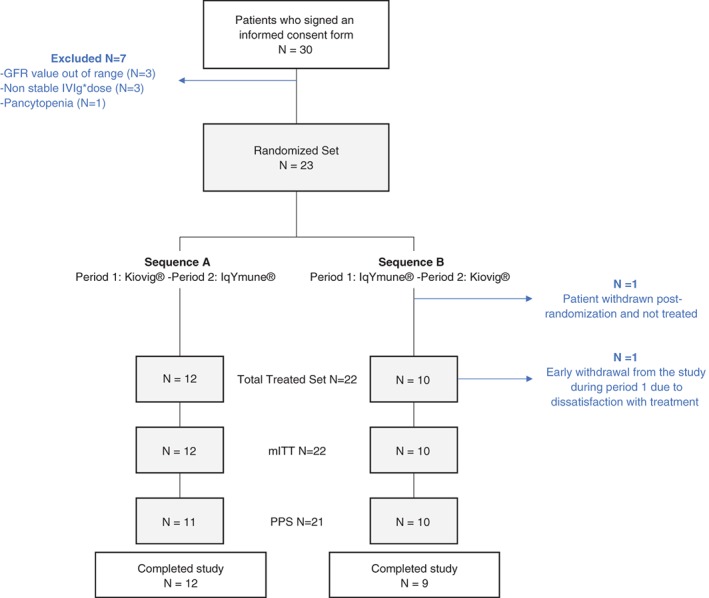
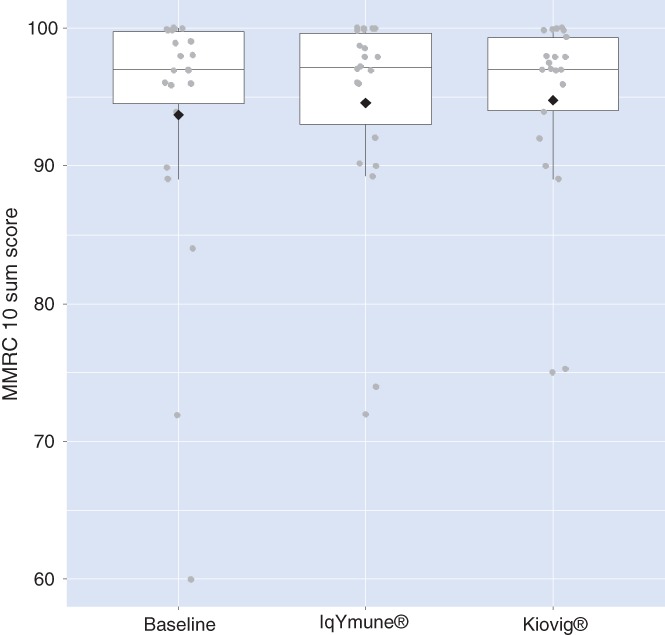
Intravenous immunoglobulin (IVIg) is the gold-standard for maintenance treatment of multifocal motor neuropathy (MMN). This phase III, randomised, double-blind, multi-centre, active-control, crossover study, aimed to evaluate the non-inferiority of IqYmune® relative to Kiovig®, primarily based on efficacy criteria. Twenty-two adult MMN patients, treated with any brand of IVIg (except Kiovig® or IqYmune®) at a stable maintenance dose within the range of 1 to 2 g/kg every 4 to 8 weeks, were randomised to receive either Kiovig® followed by IqYmune®, or IqYmune® followed by Kiovig®. Each product was administered for 24 weeks. The primary endpoint was the difference between IqYmune® and Kiovig® in mean assessments of modified Medical Research Council (MMRC) 10 sum score (strength of 5 upper-limb and 5 lower-limb muscle groups, on both sides, giving a score from 0 to 100) during the evaluation period (non-inferiority margin of Δ = 2). A linear mixed model analysis demonstrated the non-inferiority of IqYmune® relative to Kiovig®, independently of the covariates (value at baseline, treatment period, and treatment sequence). The estimated "IqYmune® - Kiovig®" difference was -0.01, with a 95% confidence interval (CI) -0.51 to 0.48. The number of adverse reactions (ARs) and the percentage of patients affected were similar for the two products: 39 ARs in 10 patients with IqYmune® vs 32 ARs in 11 patients with Kiovig®. No thromboembolic events nor haemolysis nor renal impairment were observed. In this first clinical trial comparing two IVIg brands for maintenance treatment of MMN, efficacy and tolerability of both brands were similar.
Keywords: IVIg; clinical trial; immunoglobulin; multifocal motor neuropathy.
© 2018 LFB. Journal of the Peripheral Nervous System published by Wiley Periodicals, Inc. on behalf of Peripheral Nerve Society.
Figures
References
-
- Van den Bergh PY, Hadden RD, Bouche P, et al. European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society – first revision. Eur J Neurol. 2010;17(3):356‐363. 10.1111/j.1468-1331.2009.02930.x. - DOI - PubMed
-
- Elovaara I, Apostolski S, van Doorn P, et al. EFNS guidelines for the use of intravenous immunoglobulin in treatment of neurological diseases: EFNS task force on the use of intravenous immunoglobulin in treatment of neurological diseases. Eur J Neurol. 2008;15(9):893‐908. 10.1111/j.1468-1331.2008.02246.x. - DOI - PubMed
-
- Léger JM, Viala K, Cancalon F, et al. Intravenous immunoglobulin as short‐ and long‐term therapy of multifocal motor neuropathy: a retrospective study of response to IVIg and of its predictive criteria in 40 patients. J Neurol Neurosurg Psychiatry. 2008;79(1):93‐96. - PubMed
-
- Krivan G, Chernyshova L, Kostyuchenko L, et al. A multicentre study on the efficacy, safety and pharmacokinetics of IqYmune®, a highly purified 10% liquid intravenous immunoglobulin, in patients with primary immune deficiency. J Clin Immunol. 2017;37:539‐547. 10.1007/s10875-017-0416-4. - DOI - PMC - PubMed
