

Imaging of Cancer Immunotherapy: Current Approaches and Future Directions
- PMID: 30457485
- PMCID: PMC6312436
- DOI: 10.1148/radiol.2018181349
Imaging of Cancer Immunotherapy: Current Approaches and Future Directions
Abstract
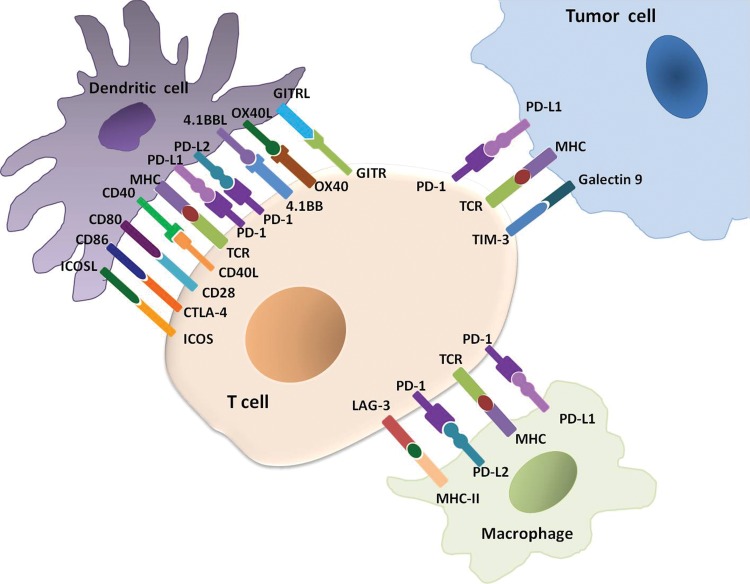
Cancer immunotherapy using immune-checkpoint inhibitors has emerged as an effective treatment option for a variety of advanced cancers in the past decade. Because of the distinct mechanisms of immunotherapy that activate the host immunity to treat cancers, unconventional immune-related phenomena are encountered in terms of tumor response and progression, as well as drug toxicity. Imaging plays an important role in objectively characterizing immune-related tumor responses and progression and in detecting and monitoring immune-related adverse events. Moreover, emerging data suggest a promise for molecular imaging that can visualize the specific target molecules involved in immune-checkpoint pathways. In this article, the background and current status of cancer immunotherapy are summarized, and the current methods for imaging evaluations of immune-related responses and toxicities are reviewed along with their limitations and pitfalls. Emerging approaches with molecular imaging are also discussed as a future direction to address unmet needs.
© RSNA, 2018.
Figures




References
-
- Allison JP, Krummel MF. The yin and yang of T cell costimulation. Science 1995;270(5238):932–933. - PubMed
-
- Hodi FS, Oble DA, Drappatz J, et al. . CTLA-4 blockade with ipilimumab induces significant clinical benefit in a female with melanoma metastases to the CNS. Nat Clin Pract Oncol 2008;5(9):557–561. - PubMed
-
- Ott PA, Hodi FS, Robert C. CTLA-4 and PD-1/PD-L1 blockade: new immunotherapeutic modalities with durable clinical benefit in melanoma patients. Clin Cancer Res 2013;19(19):5300–5309. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
