

TIMP-1 is a novel serum biomarker for the diagnosis of colorectal cancer: A meta-analysis
- PMID: 30458003
- PMCID: PMC6245680
- DOI: 10.1371/journal.pone.0207039
TIMP-1 is a novel serum biomarker for the diagnosis of colorectal cancer: A meta-analysis
Abstract
Purpose: Tissue inhibitor of metalloproteinase-1 (TIMP-1) is a glycoprotein involved in cell survival and tumorigenesis. There have been some promising results regarding the diagnostic value of TIMP-1 for patients with colorectal cancer (CRC). The aim of the present study was to assess the diagnostic accuracy and clinical utility of serum TIMP-1 in CRC patients through meta-analysis.
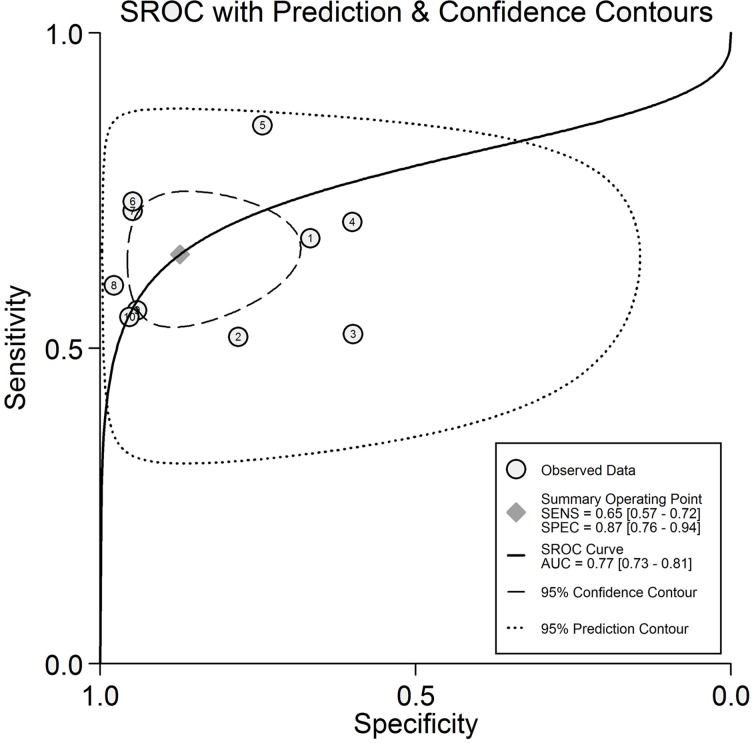
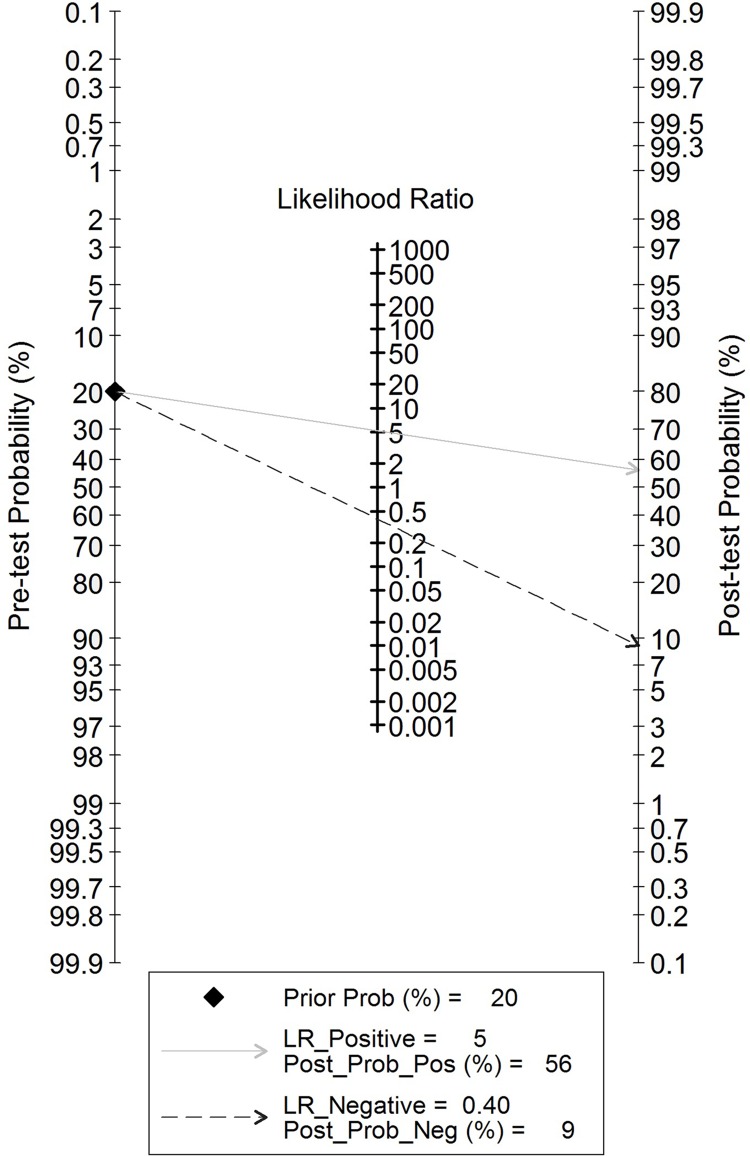
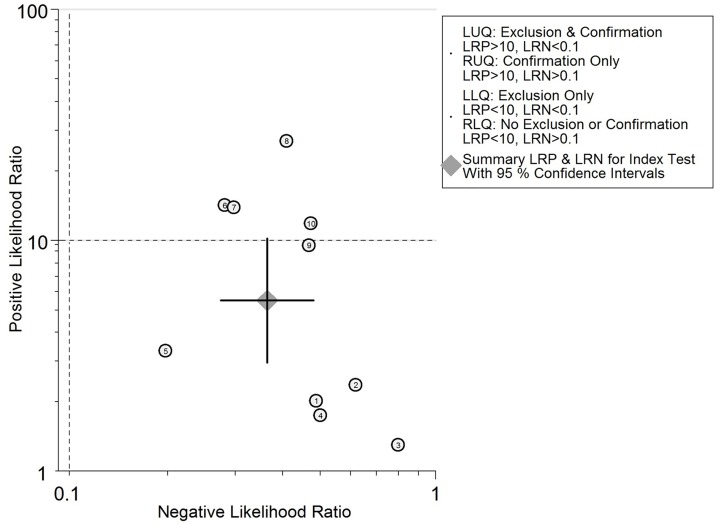
Methods: A systematic search of online databases was performed to collect eligible studies. The pooled sensitivity, specificity, diagnostic odds ratio (DOR), and summary receiver operator characteristic (SROC) curve were generated from accuracy data using the random-effects model. Fagan's nomogram and the likelihood matrix were applied to estimate the clinical utility of TIMP-1.
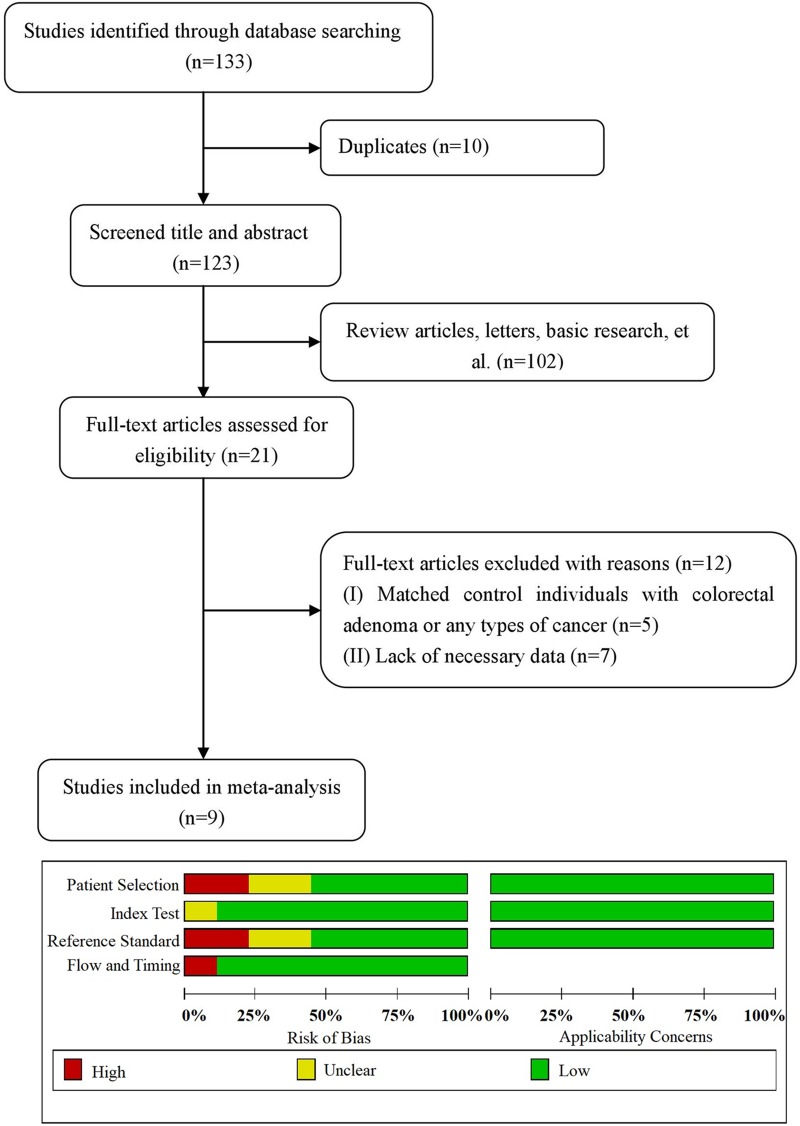
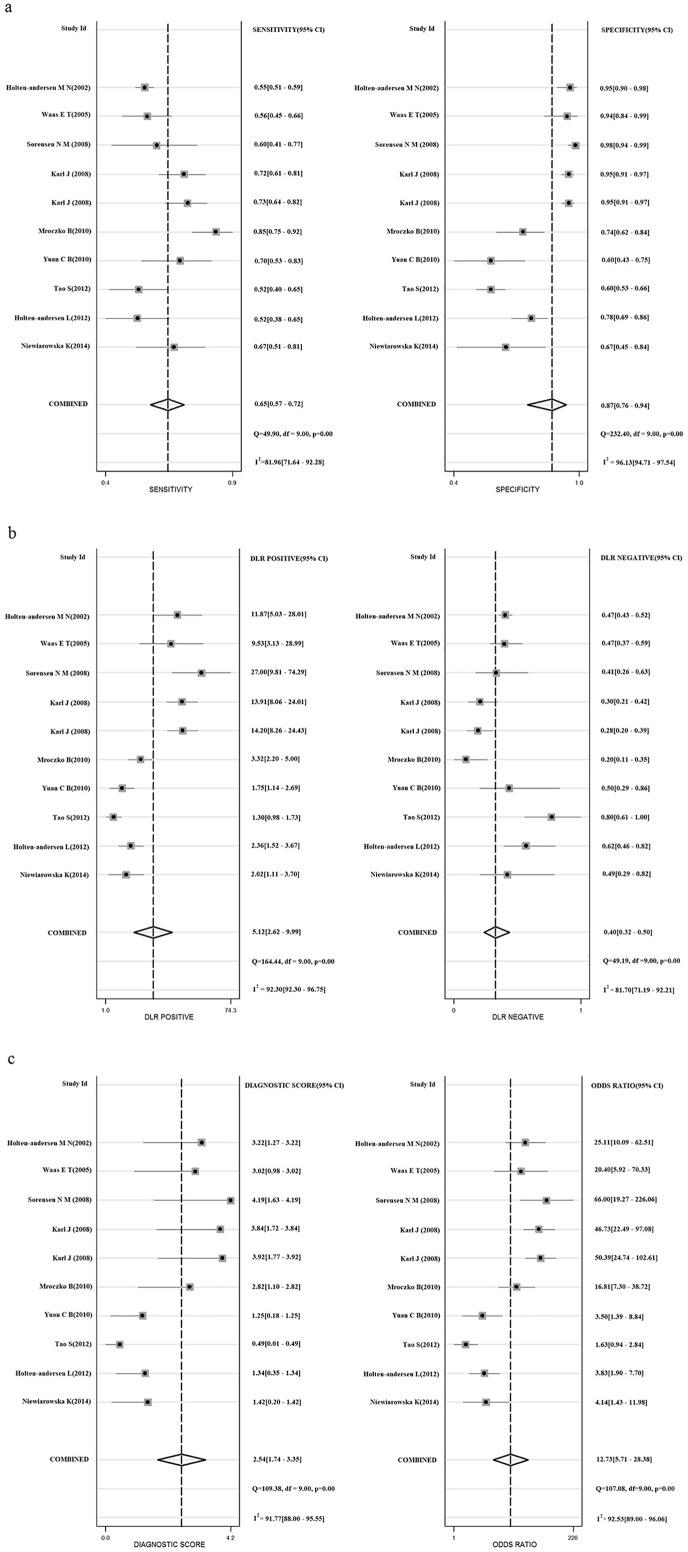
Results: A total of 9 eligible studies with 1886 patients were included. Among the patients, 819 were pathologically diagnosed with CRC, whereas 1067 did not have adenomas or other cancers. The overall sensitivity, specificity, and DOR of TIMP-1 for the diagnosis of CRC were 0.65 (95% confidence interval (CI): 0.57-0.72), 0.87 (95% CI: 0.76-0.94), and 12.73 (95% CI 5.71-28.38), respectively. The area under the SROC was 0.77 (95% CI, 0.73-0.81), suggesting the potential diagnostic value of TIMP-1 in CRC patients. Among patients with a pretest CRC probability of 20%, posttest probabilities were 56% and 9% for positive and negative TIMP-1 results, respectively.
Conclusions: TIMP-1 expression exhibits an upper moderate diagnostic value in CRC, and TIMP-1 assessment may be useful as a noninvasive screening tool for CRC in clinical practice.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Giaginis C, Nikiteas N, Margeli A, Tzanakis N, Rallis G, Kouraklis G, et al. Serum tissue inhibitor of metalloproteinase 1 and 2 (TIMP-1 and TIMP-2) levels in colorectal cancer patients: associations with clinicopathological variables and patient survival. International Journal of Biological Markers, 2010, 24(4):245–252. - PubMed
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. Ca A Cancer Journal for Clinicians, 2015, 65(2):87–108. 10.3322/caac.21262 - DOI - PubMed
-
- Hundt S, Haug U, Brenner H. Blood markers for early detection of colorectal cancer: a systematic review. Cancer Epidemiol Biomarkers Prev, 2007, 16(10):1935–1953. 10.1158/1055-9965.EPI-06-0994 - DOI - PubMed
-
- Nielsen HJ, Brünner N, Jorgensen LN, Olsen J, Rahr HB, Thygesen K, et al. Plasma TIMP-1 and CEA in detection of primary colorectal cancer: a prospective, population based study of 4509 high-risk individuals. Scand J Gastroenterol, 2011, 46(1):60–69. 10.3109/00365521.2010.513060 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
