

High-Deductible Insurance and Delay in Care for the Macrovascular Complications of Diabetes
- PMID: 30458499
- PMCID: PMC6934173
- DOI: 10.7326/M17-3365
High-Deductible Insurance and Delay in Care for the Macrovascular Complications of Diabetes
Abstract
Background: Little is known about the long-term effects of high-deductible insurance on care for chronic medical conditions.
Objective: To determine whether a transition from low-deductible to high-deductible insurance is associated with delayed medical care for macrovascular complications of diabetes.
Design: Observational longitudinal comparison of matched groups.
Setting: A large national health insurer during 2003 to 2012.
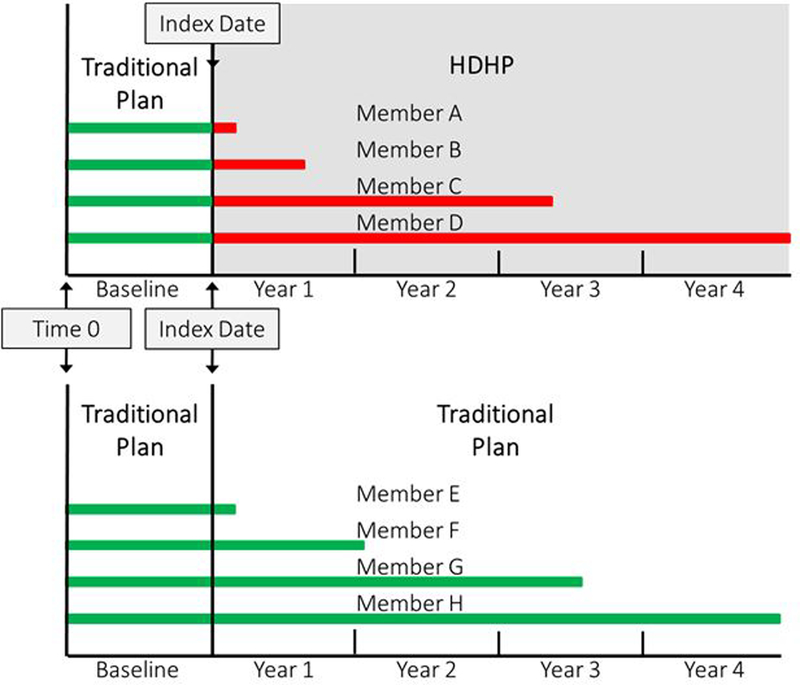
Participants: The intervention group comprised 33 957 persons with diabetes who were continuously enrolled in low-deductible (≤$500) insurance plans during a baseline year followed by up to 4 years in high-deductible (≥$1000) plans. The control group included 294 942 persons with diabetes who were enrolled in low-deductible plans contemporaneously with matched intervention group members.
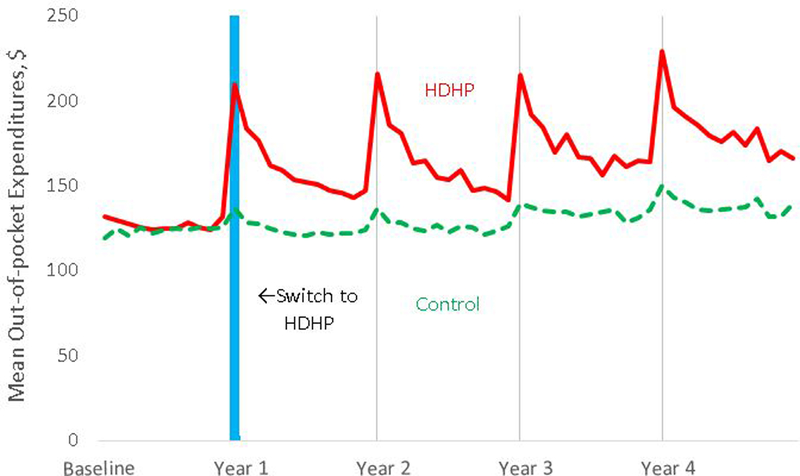
Intervention: Employer-mandated transition to a high-deductible plan.
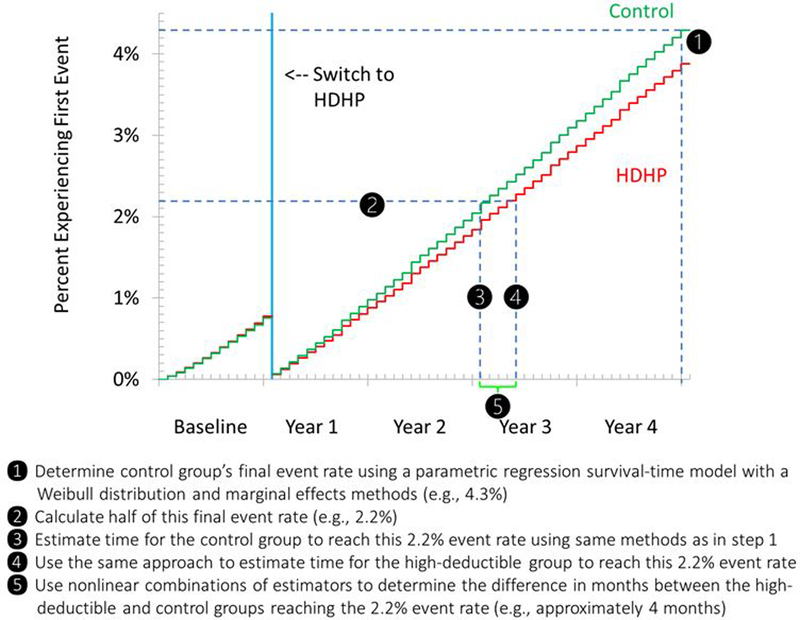
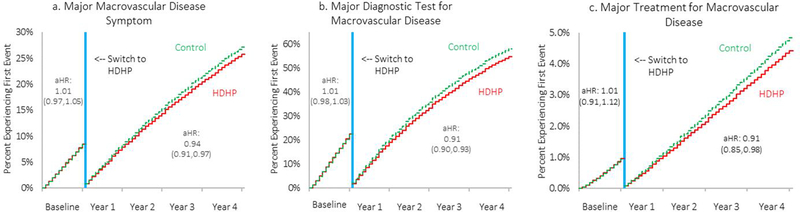
Measurements: The number of months it took for persons in each study group to seek care for their first major macrovascular symptom, have their first major diagnostic test for macrovascular disease, and have their first major procedure-based treatment was determined. Between-group differences in time to reach a midpoint event rate were then calculated.
Results: No baseline differences were found between groups. During follow-up, the delay for the high-deductible group was 1.5 months (95% CI, 0.8 to 2.3 months) for seeking care for the first major symptom, 1.9 months (CI, 1.4 to 2.3 months) for the first diagnostic test, and 3.1 months (CI, 0.5 to 5.8 months) for the first procedure-based treatment.
Limitation: Health outcomes were not examined.
Conclusion: Among persons with diabetes, mandated enrollment in a high-deductible insurance plan was associated with delays in seeking care for the first major symptoms of macrovascular disease, the first diagnostic test, and the first procedure-based treatment.
Primary funding source: National Institute of Diabetes and Digestive and Kidney Diseases.
Figures
Comment in
-
Switching to High-Deductible Health Plans: It Is Going to Be a Bumpy Ride.Ann Intern Med. 2018 Dec 18;169(12):879-880. doi: 10.7326/M18-2825. Epub 2018 Nov 20. Ann Intern Med. 2018. PMID: 30458466 No abstract available.
-
High-Deductible Insurance and Delay in Care.Ann Intern Med. 2019 Aug 6;171(3):226. doi: 10.7326/L19-0204. Ann Intern Med. 2019. PMID: 31382281 No abstract available.
-
High-Deductible Insurance and Delay in Care.Ann Intern Med. 2019 Aug 6;171(3):226. doi: 10.7326/L19-0205. Ann Intern Med. 2019. PMID: 31382282 No abstract available.
References
-
- Fox CS, Sullivan L, D’Agostino RB Sr, Wilson PW; Framingham Heart Study. The significant effect of diabetes duration on coronary heart disease mortality: the Framingham Heart Study. Diabetes Care. 2004;27:704–8. [PMID: 14988289] - PubMed
-
- Hu FB, Stampfer MJ, Solomon CG, Liu S, Willett WC, Speizer FE, et al. The impact of diabetes mellitus on mortality from all causes and coronary heart disease in women: 20 years of follow-up. Arch Intern Med. 2001;161:1717–23. [PMID: 11485504] - PubMed
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, et al. ; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–6. [PMID: 19171871] doi: 10.1161/CIRCULATIONAHA.108.191259 - DOI - PubMed
-
- Selvin E, Coresh J, Brancati FL. The burden and treatment of diabetes in elderly individuals in the U.S. Diabetes Care. 2006;29:2415–9. [PMID: 17065677] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical