

Prognostic models for intracerebral hemorrhage: systematic review and meta-analysis
- PMID: 30458727
- PMCID: PMC6247734
- DOI: 10.1186/s12874-018-0613-8
Prognostic models for intracerebral hemorrhage: systematic review and meta-analysis
Abstract
Background: Prognostic tools for intracerebral hemorrhage (ICH) patients are potentially useful for ascertaining prognosis and recommended in guidelines to facilitate streamline assessment and communication between providers. In this systematic review with meta-analysis we identified and characterized all existing prognostic tools for this population, performed a methodological evaluation of the conducting and reporting of such studies and compared different methods of prognostic tool derivation in terms of discrimination for mortality and functional outcome prediction.
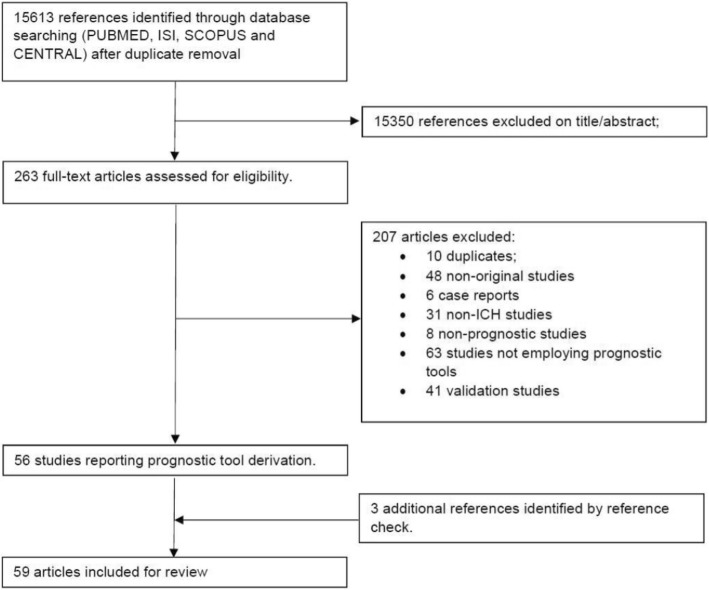
Methods: PubMed, ISI, Scopus and CENTRAL were searched up to 15th September 2016, with additional studies identified using reference check. Two reviewers independently extracted data regarding the population studied, process of tool derivation, included predictors and discrimination (c statistic) using a predesignated spreadsheet based in the CHARMS checklist. Disagreements were solved by consensus. C statistics were pooled using robust variance estimation and meta-regression was applied for group comparisons using random effect models.
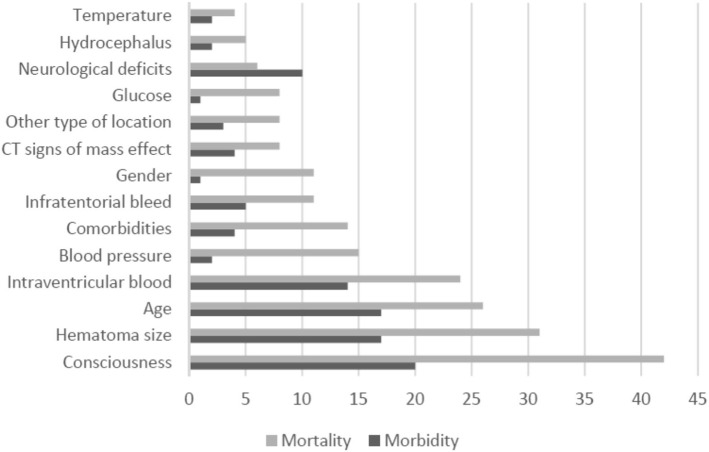
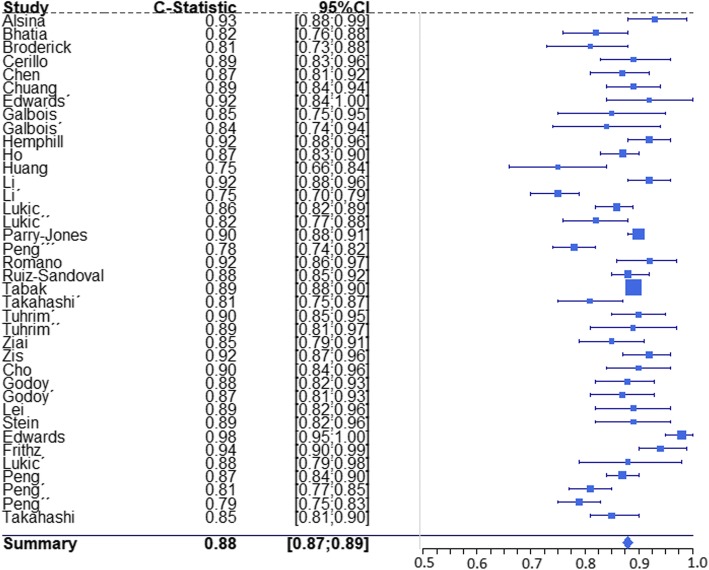
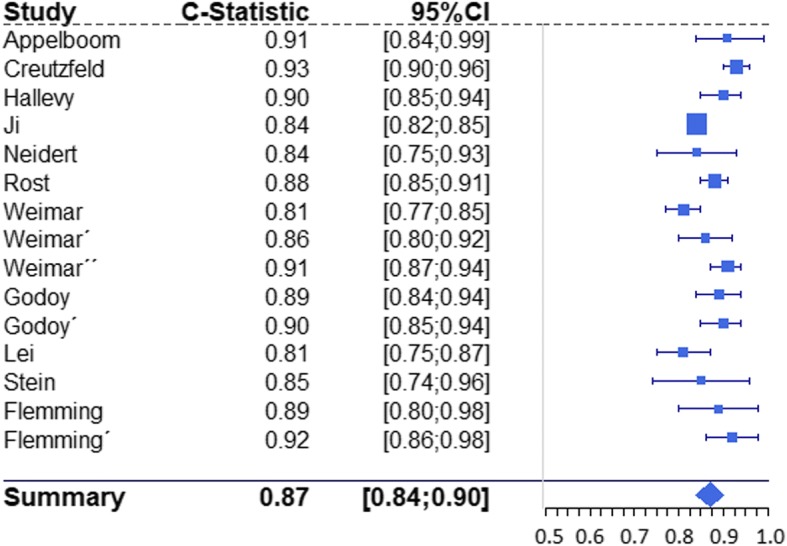
Results: Fifty nine studies were retrieved, including 48,133 patients and reporting on the derivation of 72 prognostic tools. Data on discrimination (c statistic) was available for 53 tools, 38 focusing on mortality and 15 focusing on functional outcome. Discrimination was high for both outcomes, with a pooled c statistic of 0.88 for mortality and 0.87 for functional outcome. Forty three tools were regression based and nine tools were derived using machine learning algorithms, with no differences found between the two methods in terms of discrimination (p = 0.490). Several methodological issues however were identified, relating to handling of missing data, low number of events per variable, insufficient length of follow-up, absence of blinding, infrequent use of internal validation, and underreporting of important model performance measures.
Conclusions: Prognostic tools for ICH discriminated well for mortality and functional outcome in derivation studies but methodological issues require confirmation of these findings in validation studies. Logistic regression based risk scores are particularly promising given their good performance and ease of application.
Keywords: Clinical prediction rules; Intracerebral hemorrhage; Morbidity; Mortality; Prognosis.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Van Asch CJJ, Luitse MJA, Rinkel GJE, Van Der Tweel I, Algra A, Klijn CJM. Incidence , case fatality , and functional outcome of intracerebral haemorrhage over time, according to age , sex , and ethnic origin : a systematic review and meta-analysis. Lancet Neurol. 2017;9(2):167–176. doi: 10.1016/S1474-4422(09)70340-0. - DOI - PubMed
-
- Hemphill JC, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46:2032–2060. doi: 10.1161/STR.0000000000000069. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
