

Integrated models of care for diabetes and hypertension in low- and middle-income countries (LMICs) : Protocol for a systematic review
- PMID: 30458841
- PMCID: PMC6247752
- DOI: 10.1186/s13643-018-0865-8
Integrated models of care for diabetes and hypertension in low- and middle-income countries (LMICs) : Protocol for a systematic review
Erratum in
-
Correction to: Integrated models of care for diabetes and hypertension in low- and middle-income countries (LMICs): Protocol for a systematic review.Syst Rev. 2019 Jan 31;8(1):36. doi: 10.1186/s13643-019-0943-6. Syst Rev. 2019. PMID: 30704523 Free PMC article.
Abstract
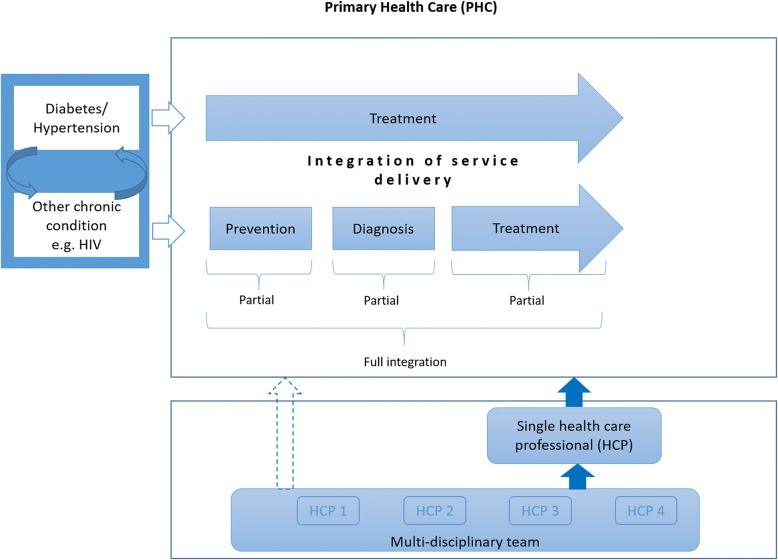
Background: In low- and middle-income countries (LMICs), the burden of non-communicable diseases (NCDs) is growing against an existing burden of other diseases such as HIV/AIDS. Integrated models of care can help address the rising burden of multi-morbidity. Although integration of care can occur at various levels and has been defined in numerous ways, our aim is to assess the effects of integration of service delivery at primary healthcare level in LMICs.
Methods: We will consider randomised controlled trials (RCTs), cluster RCTs, non-randomised trials, controlled before-after studies and interrupted time series that examine integrated models of care among people with multi-morbidities, of which diabetes or hypertension is one, living in LMICs. We will compare fully integrated models of care to stand-alone care, partially integrated models of care to stand-alone care and fully integrated models to partially integrated models of care. Primary outcomes include all-cause mortality, disease-specific morbidity, HbA1c, systolic blood pressure and cholesterol levels. Secondary outcomes include access to care, retention in care, adherence, continuity of care, quality of care and cost of care. We will conduct a comprehensive search in the following databases: MEDLINE, EMBASE, the Cochrane Central Register of Control Trials, LILACS, Africa-Wide Information, CINAHL and Web of Science. In addition, we will search trial registries, relevant conference abstracts and check references lists of included studies. Selection of studies, data extraction and assessment of risk of bias will be performed independently by two review authors. We will resolve discrepancies through discussion with a third author. We will contact study authors in case of missing data. If included studies are sufficiently homogenous, we will pool results in a meta-analysis. Clinical heterogeneity related to the population, intervention, outcomes and context will be documented in table format and explored through subgroup analysis. We will assess χ 2 and I 2 tests for statistical heterogeneity. We will use GRADE to make judgements about the certainty of evidence and present findings in a summary of findings table.
Discussion: In light of limited evidence on the provision of comprehensive care for diabetes and hypertension, and its comorbidity in LMCIs, we believe that the findings of this systematic review will provide a synthesis of evidence on effective models of integrated care for diabetes and hypertension and their comorbidities at primary healthcare level. This will enable policy-makers to device policies and programs that are evidence informed.
Systematic review registration: PROSPERO CRD42018099314 .
Keywords: Diabetes; Hypertension; Integrated care; Low- and middle-income countries; Multi-morbidity; Non-communicable diseases.
Conflict of interest statement
Authors’ information
JUN and AR are senior researchers at the Centre for Evidence-based Healthcare (CEBHC), Division of Epidemiology and Biostatistics, Department of Global Health, Stellenbosch University. TY is the director of the CEBHC and head of Division of Epidemiology and Biostatistics, Department of Global Health, Stellenbosch University. CMB is clinician and lecturer at the College of Medicine and Health Sciences, University of Rwanda. JJM is the director of GRADE Centre Freiburg and co-director of Cochrane Germany.
Ethics approval and consent to participate
Since the current systematic review and meta-analysis will not involve any human participants, no ethics approval is needed as well as the consent to participate.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Effects of integrated models of care for diabetes and hypertension in low-income and middle-income countries: a systematic review and meta-analysis.BMJ Open. 2021 Jul 12;11(7):e043705. doi: 10.1136/bmjopen-2020-043705. BMJ Open. 2021. PMID: 34253658 Free PMC article.
-
Integration of care for hypertension and diabetes: a scoping review assessing the evidence from systematic reviews and evaluating reporting.BMC Health Serv Res. 2018 Jun 20;18(1):481. doi: 10.1186/s12913-018-3290-8. BMC Health Serv Res. 2018. PMID: 29925356 Free PMC article.
-
The effectiveness of interventions to improve uptake and retention of HIV-infected pregnant and breastfeeding women and their infants in prevention of mother-to-child transmission care programs in low- and middle-income countries: protocol for a systematic review and meta-analysis.Syst Rev. 2015 Nov 3;4:144. doi: 10.1186/s13643-015-0136-x. Syst Rev. 2015. PMID: 26525141 Free PMC article.
-
The effect of depression management on diabetes and hypertension outcomes in low- and middle-income countries: a systematic review protocol.Syst Rev. 2018 Dec 5;7(1):223. doi: 10.1186/s13643-018-0896-1. Syst Rev. 2018. PMID: 30518434 Free PMC article.
-
Interventions to reduce ambient particulate matter air pollution and their effect on health.Cochrane Database Syst Rev. 2019 May 20;5(5):CD010919. doi: 10.1002/14651858.CD010919.pub2. Cochrane Database Syst Rev. 2019. PMID: 31106396 Free PMC article.
Cited by
-
Contemporary issues and new challenges in chronic kidney disease amongst people living with HIV.AIDS Res Ther. 2020 Mar 16;17(1):11. doi: 10.1186/s12981-020-00266-3. AIDS Res Ther. 2020. PMID: 32178687 Free PMC article. Review.
-
Effects of integrated models of care for diabetes and hypertension in low-income and middle-income countries: a systematic review and meta-analysis.BMJ Open. 2021 Jul 12;11(7):e043705. doi: 10.1136/bmjopen-2020-043705. BMJ Open. 2021. PMID: 34253658 Free PMC article.
-
Correction to: Integrated models of care for diabetes and hypertension in low- and middle-income countries (LMICs): Protocol for a systematic review.Syst Rev. 2019 Jan 31;8(1):36. doi: 10.1186/s13643-019-0943-6. Syst Rev. 2019. PMID: 30704523 Free PMC article.
-
Stakeholder perspectives on the barriers and facilitators to integrating cardiovascular disease and diabetes management at primary care in Kenya.PLOS Glob Public Health. 2025 Jul 3;5(7):e0004164. doi: 10.1371/journal.pgph.0004164. eCollection 2025. PLOS Glob Public Health. 2025. PMID: 40608702 Free PMC article.
-
The effects of an innovative integrated care intervention in Brazil on local health service use by dependent older people.BMC Health Serv Res. 2022 Feb 11;22(1):176. doi: 10.1186/s12913-022-07552-y. BMC Health Serv Res. 2022. PMID: 35144611 Free PMC article.
References
-
- WHO . Non-Communicable diseases factsheet. 2017.
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
-
- NCD Alliance . Tackling non-communicable diseases in workplace settings in low- and middle-income countries. A CALL TO ACTION AND PRACTICAL GUIDANCE. Non- Communicable diseases (NCD) Alliance. 2017.
-
- IDF diabetes Atlas 8th edition. https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/134-i.... Accessed 14 Mar 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
