

Metabolomics and transcriptomics pathway approach reveals outcome-specific perturbations in COPD
- PMID: 30459441
- PMCID: PMC6244246
- DOI: 10.1038/s41598-018-35372-w
Metabolomics and transcriptomics pathway approach reveals outcome-specific perturbations in COPD
Abstract
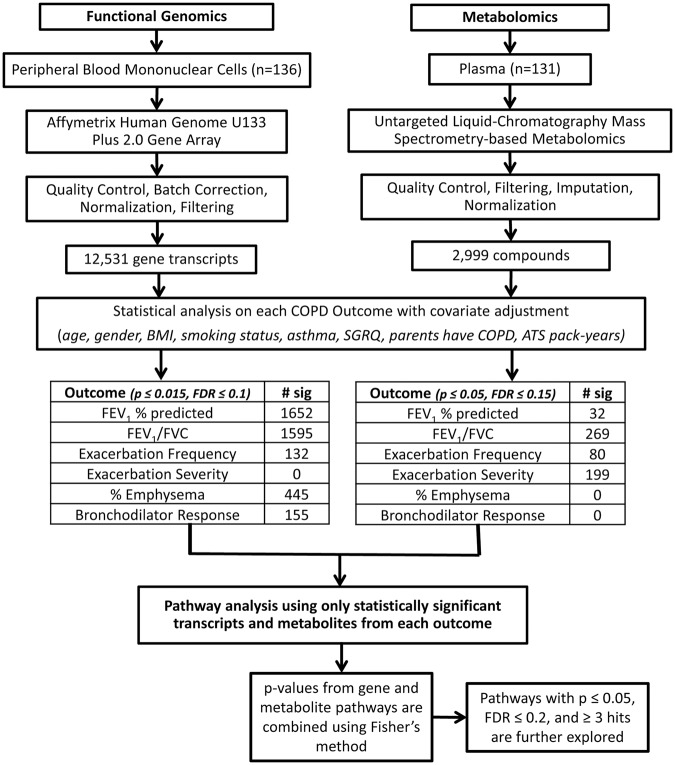
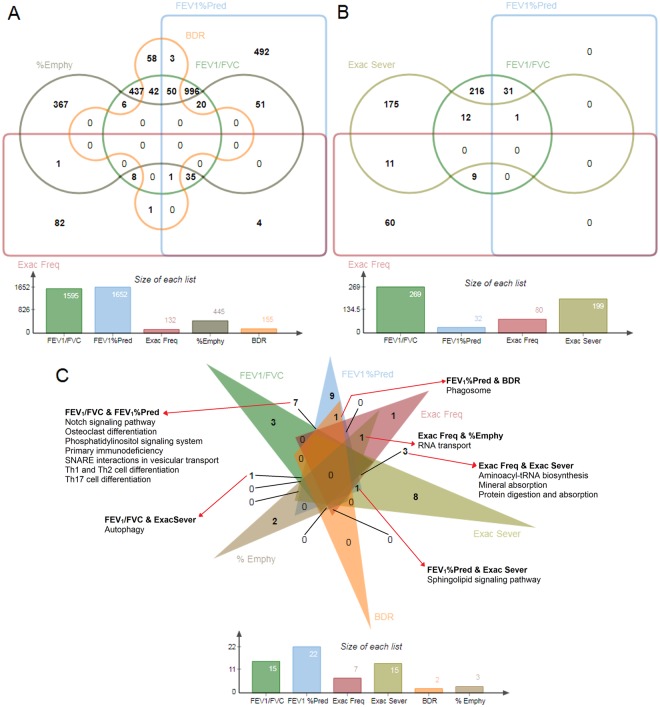
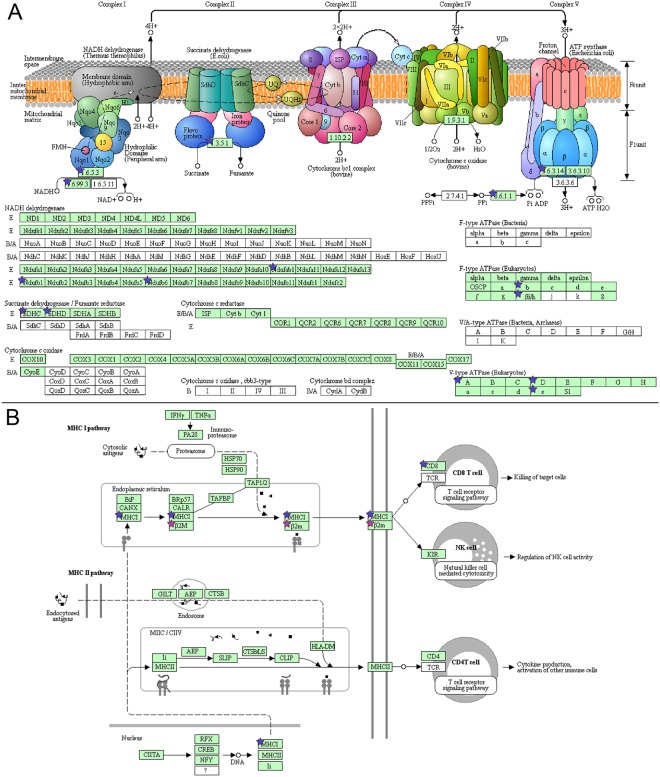
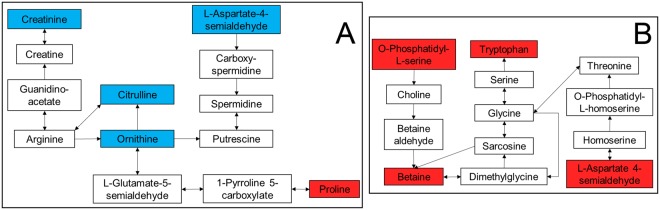
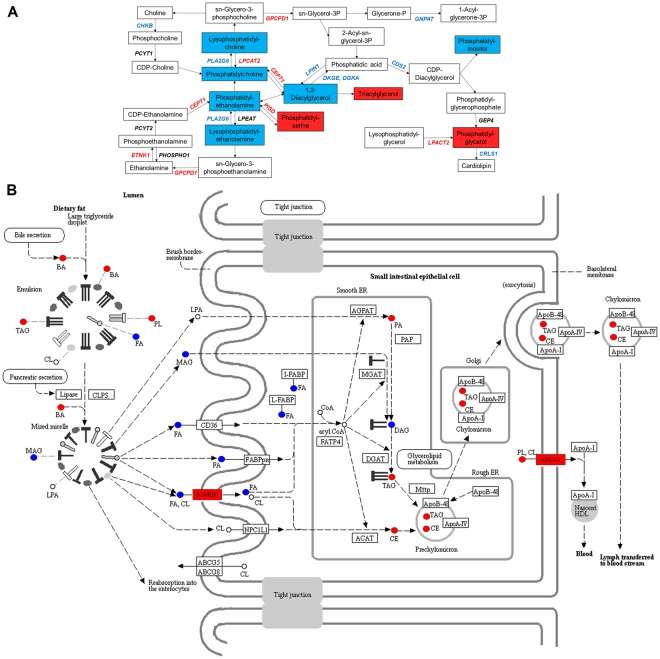
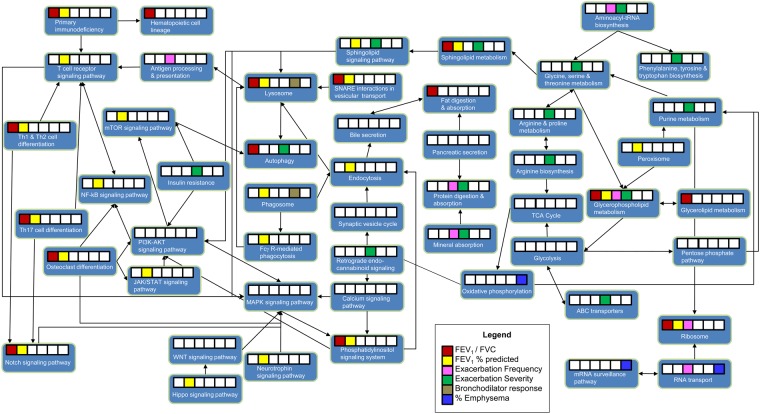
Chronic obstructive pulmonary disease (COPD) comprises multiple phenotypes such as airflow obstruction, emphysema, and frequent episodes of acute worsening of respiratory symptoms, known as exacerbations. The goal of this pilot study was to test the usefulness of unbiased metabolomics and transcriptomics approaches to delineate biological pathways associated with COPD phenotypes and outcomes. Blood was collected from 149 current or former smokers with or without COPD and separated into peripheral blood mononuclear cells (PBMC) and plasma. PBMCs and plasma were analyzed using microarray and liquid chromatography mass spectrometry, respectively. Statistically significant transcripts and compounds were mapped to pathways using IMPaLA. Results showed that glycerophospholipid metabolism was associated with worse airflow obstruction and more COPD exacerbations. Sphingolipid metabolism was associated with worse lung function outcomes and exacerbation severity requiring hospitalizations. The strongest associations between a pathway and a certain COPD outcome were: fat digestion and absorption and T cell receptor signaling with lung function outcomes; antigen processing with exacerbation frequency; arginine and proline metabolism with exacerbation severity; and oxidative phosphorylation with emphysema. Overlaying transcriptomic and metabolomics datasets across pathways enabled outcome and phenotypic differences to be determined. Findings are relevant for identifying molecular targets for animal intervention studies and early intervention markers in human cohorts.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- CDC Chronic obstructive pulmonary disease among adults—United States, 2011. Morb. Mortal. Weekly Rep. 2012;61:938–943. - PubMed
-
- GBD 2015 Chronic Respiratory Disease Collaborators Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. 2017;5:691–706. doi: 10.1016/s2213-2600(17)30293-x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 RR025780/RR/NCRR NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL095432/HL/NHLBI NIH HHS/United States
- R01 HL 095432/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)/International
- U01 HL089856/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
