

Comparison of the genomic background of MET-altered carcinomas of the lung: biological differences and analogies
- PMID: 30459450
- PMCID: PMC6760650
- DOI: 10.1038/s41379-018-0182-8
Comparison of the genomic background of MET-altered carcinomas of the lung: biological differences and analogies
Abstract
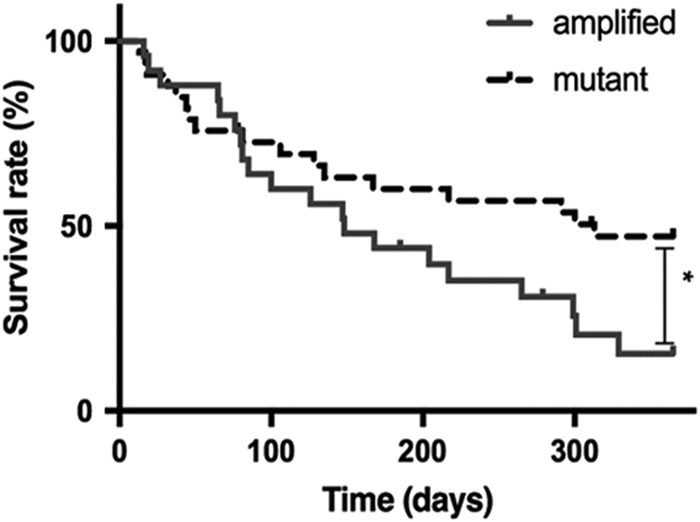
Although non-small-cell lung cancer is a leading cause of cancer-related deaths, the molecular characterization and classification of its genetic alterations has drastically changed treatment options and overall survival within the last few decades. In particular, tyrosine kinase inhibitors targeting specific molecular alterations, among other MET, have greatly improved the prognosis of non-small-cell lung cancer patients. Here, we compare the genomic background of a subset of non-small-cell lung cancer cases harboring either a MET high-level amplification (n = 24) or a MET exon 14 skipping mutation (n = 26), using next-generatison sequencing, fluorescence in situ hybridization, immunohistochemistry, and Nanostring nCounter® technology. We demonstrate that the MET-amplified cohort shows a higher genetic instability, compared with the mutant cohort (p < 0.001). Furthermore, MET mutations occur at high allele frequency and in the presence of co-occurring TP53 mutations (n = 7), as well as MDM2 (n = 7), CDK4 (n = 6), and HMGA2 (n = 5) co-amplifications. No other potential driver mutation has been detected. Conversely, in the MET-amplified group, we identify co-occurring pathogenic NRAS and KRAS mutations (n = 5) and a significantly higher number of TP53 mutations, compared with the MET-mutant cohort (p = 0.048). Of note, MET amplifications occur more frequently as subclonal events. Interestingly, despite the significantly (p = 0.00103) older age at diagnosis of stage IIIb/IV of MET-mutant patients (median 77 years), compared with MET high-level amplified patients (median 69 years), MET-mutant patients with advanced-stage tumors showed a significantly better prognosis at 12 months (p = 0.04). In conclusion, the two groups of MET genetic alterations differ, both clinically and genetically: our data strongly suggest that MET exon 14 skipping mutations represent an early driver mutation. In opposition, MET amplifications occur usually in the background of other strong genetic events and therefore MET amplifications should be interpreted in the context of each tumor's genetic background, rather than as an isolated driver event, especially when considering MET-specific treatment options.
Conflict of interest statement
HCR received consulting and lecture fees from Abbvie, Astra-Zeneca, Vertex and Merck. HCR received research funding from Gilead Pharmaceuticals.
Figures
References
-
- World Health Organization Classification of Tumours. Tumours of the Lung. In: Travis WD, Brambilla E, Müller-Hermelink K Harris CC, editors, Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. 3rd edn. Lyon, France: IARCPress, 2004, p12–25.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
