

Case Reports
doi: 10.1259/bjrcr.20150370.
eCollection 2016.
Actinomycotic brain abscess
Affiliations
- PMID: 30460021
- PMCID: PMC6243313
- DOI: 10.1259/bjrcr.20150370
Item in Clipboard
Case Reports
Actinomycotic brain abscess
BJR Case Rep.
.
Abstract
Actinomycosis is caused by Gram-positive filamentous anaerobic organisms of genus Actinomyces, which are commensals of mucosal membranes of the oropharyngeal cavity, and gastrointestinal and genitourinary tracts. Central nervous system involvement is rare and may present as cerebral abscess, meningitis, meningoencephalitis, subdural empyema or epidural abscess. The radiological appearances of actinomycotic brain abscesses are not well recognized. Here, we present the characteristic imaging features of an actinomycotic brain abscess.
Figures
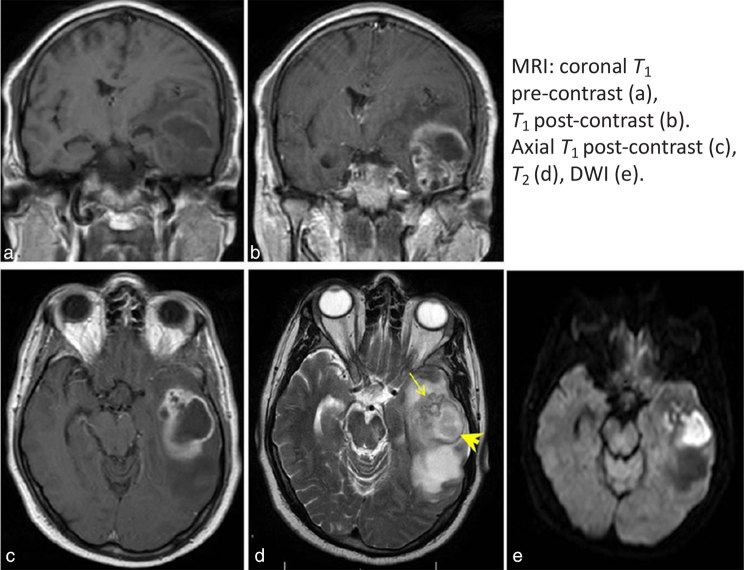
There is a large, peripherally enhancing thick-walled lesion in the left temporal lobe. The lesion comprises a larger cavity posteriorly and grape-like clustering anteriorly (arrow). The wall is T2 hypointense and T1 hyperintense (arrowhead). The contents of the lesion show restricted diffusion, which is consistent with an abscess. The diagnosis is suggested by the grape-like cluster pattern with a T2 hypointense wall, which is a characteristic feature of an actinomycotic abscess. DWI, diffusion-weighted imaging.
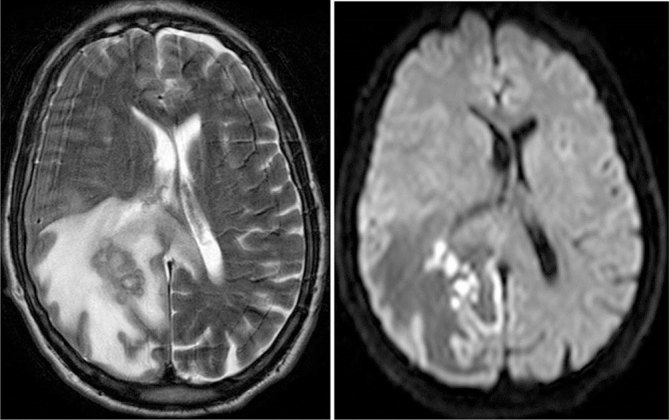
Axial T2 and diffusion-weighted MRI in a 60-year-old male with an actinomycotic brain abscess in the right parietal lobe with surrounding oedema. There is grape-like clustering with a T2 hypointense thick wall. The contents show restricted diffusion.
References
-
- Omuro AM, Leite CC, Mokhtari K, Delattre JY. Pitfalls in the diagnosis of brain tumours. Lancet Neurol 2006; 5: 937–48. - PubMed
-
- Wang S, Wolf RL, Woo JH, Wang J, O'Rourke DM, Roy S, et al. . Actinomycotic brain infection: registered diffusion, perfusion MR imaging and MR spectroscopy. Neuroradiology 2006; 48: 346–50. - PubMed
-
- Heo SH, Shin SS, Kim JW, Lim HS, Seon HJ, Jung SI, et al. . Imaging of actinomycosis in various organs: a comprehensive review. Radiographics 2014; 34: 19–33. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
