Respiratory mechanics in patients with acute respiratory distress syndrome
- PMID: 30460256
- PMCID: PMC6212350
- DOI: 10.21037/atm.2018.08.32
Respiratory mechanics in patients with acute respiratory distress syndrome
Abstract
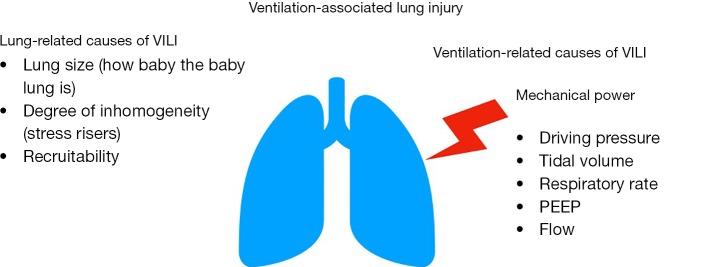
Despite the recognition of its iatrogenic potential, mechanical ventilation remains the mainstay of respiratory support for patients with acute respiratory distress syndrome (ARDS). The low volume ventilation has been recognized as the only method to reduce mortality of ARDS patients and plateau pressure as the lighthouse for delivering safe ventilation. Recent investigations suggest that a ventilation based on lung mechanics (tidal ventilation tailored to the available lung volume able to receive it, i.e., driving pressure) is a successful approach to improve outcome. However, currently available bedside mechanical variables do not consider regional mechanical properties of ARDS affected lungs, which include the role of local stress risers at the boundaries of areas with different aeration. A unifying approach considers lung-related causes and ventilation-related causes of lung injury. These last may be incorporated in the mechanical power (i.e., amount of mechanical energy transferred per unit of time). Ventilation-induced lung injury (which includes the self-inflicted lung injury of a spontaneously breathing patient) can therefore be prevented by the adoption of measures promoting an increase of ventilable lung and its homogeneity and by delivering lower levels of mechanical power. Prone position promotes lung homogeneity without increasing the delivered mechanical power. This review describes the recent developments on respiratory mechanics in ARDS patients, providing both bedside and research insights from the most updated evidence.
Keywords: Respiratory mechanics; acute respiratory distress syndrome (ARDS); ventilator-induced lung injury (VILI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures