

Mechanical ventilation and respiratory monitoring during extracorporeal membrane oxygenation for respiratory support
- PMID: 30460260
- PMCID: PMC6212363
- DOI: 10.21037/atm.2018.10.11
Mechanical ventilation and respiratory monitoring during extracorporeal membrane oxygenation for respiratory support
Abstract
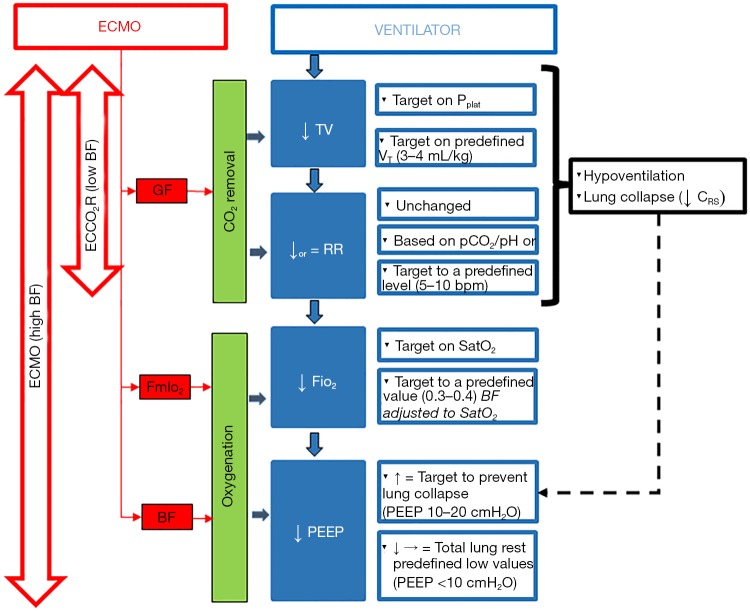
Over the past decade, the use of veno-venous extracorporeal membrane oxygenation (VV-ECMO) for respiratory support has widely expanded as a treatment strategy for patients with acute respiratory distress syndrome (ARDS). Despite considerable attention has been given to the indications, the timing and the management of patients undergoing ECMO for refractory respiratory hypoxemic failure, little is known regarding the management of mechanical ventilation (MV) in this group of patients. ECMO enables to minimize ventilatory induced lung injury (VILI) and it has been successfully used as rescue therapy in patients with ARDS when conventional ventilator strategies have failed. However, literature is lacking regarding the best strategies and MV settings, including positive end expiratory pressure (PEEP), tidal volume (VT), respiratory rate (RR) and plateau pressure (PPLAT). The aim of this review is to summarize current evidence, the rationale and provide recommendations about the best ventilator strategy to adopt in patients with ARDS undergoing VV-ECMO support.
Keywords: Mechanical ventilation (MV); acute respiratory distress syndrome (ARDS); extracorporeal membrane oxygenation (ECMO); positive end expiratory pressure (PEEP).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- ARDS Definition Task Force , Ranieri V, Rubenfeld G, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012;307:2526-33. - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 2009;374:1351-63. 10.1016/S0140-6736(09)61069-2 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous