

Should we titrate positive end-expiratory pressure based on an end-expiratory transpulmonary pressure?
- PMID: 30460265
- PMCID: PMC6212349
- DOI: 10.21037/atm.2018.08.22
Should we titrate positive end-expiratory pressure based on an end-expiratory transpulmonary pressure?
Abstract
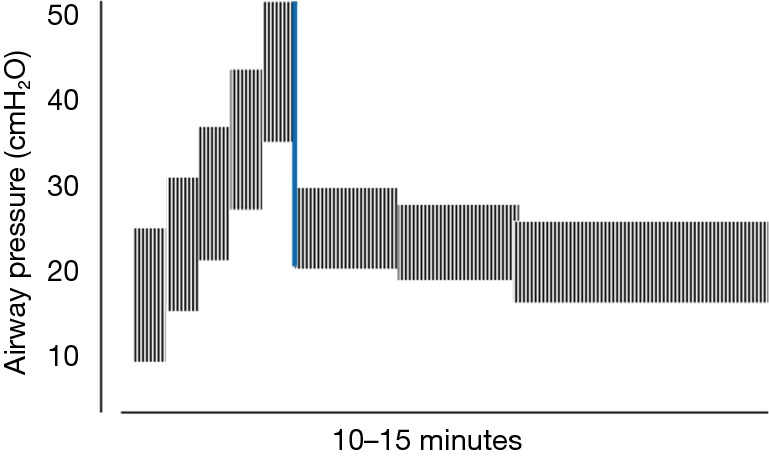
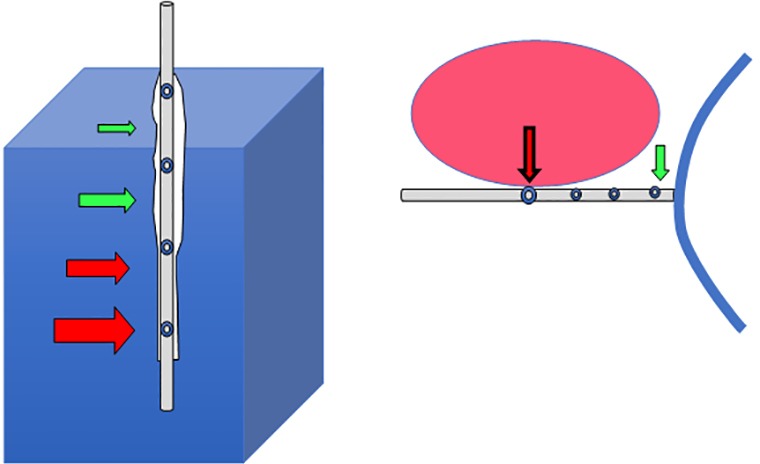
Arguments continue to swirl regarding the need for and best method of positive end-expiratory pressure (PEEP) titration. An appropriately conducted decremental method that uses modest peak pressures for the recruiting maneuver (RM), a lung protective tidal excursion, relatively small PEEP increments and appropriate timing intervals is currently the most logical and attractive option, particularly when the esophageal balloon pressure (Pes) is used to calculate transpulmonary driving pressures relevant to the lung. The setting of PEEP by the Pes-guided end-expiratory pressure at the 'polarity transition' point of the transmural end-expiratory pressure is quite relevant to the locale of the esophageal balloon catheter. Its desirability, however, is limited by its tendency to encourage PEEP levels that are higher than most other PEEP titration methods. These Pes-set PEEP values promote higher mean airway pressures and are likely to be unnecessary when small tidal driving pressures are in use. Because high airway pressures increase global lung stress and risk hemodynamic compromise, the Pes-determined PEEP would seem associated with a relatively high hazard to benefit ratio for many patients.
Keywords: Recruitment; esophageal pressure; mechanical ventilation; open lung, transpulmonary pressure; positive end-expiratory pressure (PEEP); recruiting maneuver (RM).
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures

Similar articles
-
How much esophageal pressure-guided end-expiratory transpulmonary pressure is sufficient to maintain lung recruitment in lavage-induced lung injury?J Trauma Acute Care Surg. 2016 Feb;80(2):302-7. doi: 10.1097/TA.0000000000000900. J Trauma Acute Care Surg. 2016. PMID: 26517781
-
Retrospective Review of Transpulmonary Pressure Guided Positive End-Expiratory Pressure Titration for Mechanical Ventilation in Class II and III Obesity.Crit Care Explor. 2022 Apr 29;4(5):e0690. doi: 10.1097/CCE.0000000000000690. eCollection 2022 May. Crit Care Explor. 2022. PMID: 35510150 Free PMC article.
-
Effects of positive end-expiratory pressure strategy in supine and prone position on lung and chest wall mechanics in acute respiratory distress syndrome.Ann Intensive Care. 2018 Sep 10;8(1):86. doi: 10.1186/s13613-018-0434-2. Ann Intensive Care. 2018. PMID: 30203117 Free PMC article.
-
Positive end-expiratory pressure.Curr Opin Crit Care. 2010 Feb;16(1):39-44. doi: 10.1097/MCC.0b013e3283354723. Curr Opin Crit Care. 2010. PMID: 19996966 Review.
-
Should we titrate ventilation based on driving pressure? Maybe not in the way we would expect.Ann Transl Med. 2018 Oct;6(19):389. doi: 10.21037/atm.2018.09.48. Ann Transl Med. 2018. PMID: 30460263 Free PMC article. Review.
Cited by
-
PEEP titration guided by transpulmonary pressure: lessons from a negative trial.J Thorac Dis. 2019 Sep;11(Suppl 15):S1957-S1962. doi: 10.21037/jtd.2019.08.03. J Thorac Dis. 2019. PMID: 31632797 Free PMC article. No abstract available.
-
Multimodal non-invasive monitoring to apply an open lung approach strategy in morbidly obese patients during bariatric surgery.J Clin Monit Comput. 2020 Oct;34(5):1015-1024. doi: 10.1007/s10877-019-00405-w. Epub 2019 Oct 25. J Clin Monit Comput. 2020. PMID: 31654282 Clinical Trial.
-
An assessment of esophageal balloon use for the titration of airway pressure release ventilation and controlled mechanical ventilation in a patient with extrapulmonary acute respiratory distress syndrome: a case report.J Med Case Rep. 2021 Aug 17;15(1):435. doi: 10.1186/s13256-021-02984-2. J Med Case Rep. 2021. PMID: 34399842 Free PMC article.
References
-
- Toung TJ, Saharia P, Mitzner WA, et al. The beneficial and harmful effects of positive end expiratory pressure. Surg Gynecol Obstet 1978;147:518-24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources