

Rethinking Bone Disease in Kidney Disease
- PMID: 30460334
- PMCID: PMC6237213
- DOI: 10.1002/jbm4.10117
Rethinking Bone Disease in Kidney Disease
Abstract
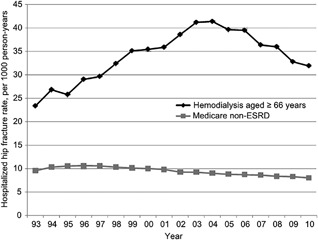
Renal osteodystrophy (ROD) is the bone component of chronic kidney disease mineral and bone disorder (CKD-MBD). ROD affects bone quality and strength through the numerous hormonal and metabolic disturbances that occur in patients with kidney disease. Collectively these disorders in bone quality increase fracture risk in CKD patients compared with the general population. Fractures are a serious complication of kidney disease and are associated with higher morbidity and mortality compared with the general population. Furthermore, at a population level, fractures are at historically high levels in patients with end-stage kidney disease (ESKD), whereas in contrast the general population has experienced a steady decline in fracture incidence rates. Based on these findings, it is clear that a paradigm shift is needed in our approach to diagnosing and managing ROD. In clinical practice, our ability to diagnose ROD and initiate antifracture treatments is impeded by the lack of accurate noninvasive methods that identify ROD type. The past decade has seen advances in the noninvasive measurement of bone quality and strength that have been studied in kidney disease patients. Below we review the current literature pertaining to the epidemiology, pathology, diagnosis, and management of ROD. We aim to highlight the pressing need for a greater awareness of this condition and the need for the implementation of strategies that prevent fractures in kidney disease patients. Research is needed for more accurate noninvasive assessment of ROD type, clinical studies of existing osteoporosis therapies in patients across the spectrum of kidney disease, and the development of CKD-specific treatments. © 2018 The Authors. JBMR Plus published by Wiley Periodicals, Inc. on behalf of the American Society for Bone and Mineral Research.
Keywords: BONE DISEASE; CKD; CKD‐MBD; ESKD; FRACTURES; OSTEOPOROSIS.
Figures
References
-
- Slatopolsky E, Delmez JA. Renal osteodystrophy. In: Avioli LV, Krane SM, editors. Metabolic bone disease and clinically related disorders. 3rd ed San Diego: Academic Press; 1998. pp. 443–64.
-
- Slatopolsky E, Gonzalez E, Martin K. Pathogenesis and treatment of renal osteodystrophy. Blood Purif. 2003; 21 (4–5): 318–26. - PubMed
-
- Moe S, Drüeke T, Cunningham J, et al. Kidney Disease: Improving Global Outcomes (KDIGO). Definition, evaluation, and classification of renal osteodystrophy: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006; 69 (11): 1945–53. - PubMed
-
- Kim SM, Long J, Montez‐Rath M, Leonard M, Chertow GM. Hip fracture in patients with non‐dialysis‐requiring chronic kidney disease. J. Bone Miner Res. 2016; 31 (10): 1803–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous