

Preventing Postoperative Delirium After Major Noncardiac Thoracic Surgery-A Randomized Clinical Trial
- PMID: 30460981
- PMCID: PMC10924437
- DOI: 10.1111/jgs.15640
Preventing Postoperative Delirium After Major Noncardiac Thoracic Surgery-A Randomized Clinical Trial
Abstract
Objectives: To assess the efficacy of haloperidol in reducing postoperative delirium in individuals undergoing thoracic surgery.
Design: Randomized double-blind placebo-controlled trial.
Setting: Surgical intensive care unit (ICU) of tertiary care center.
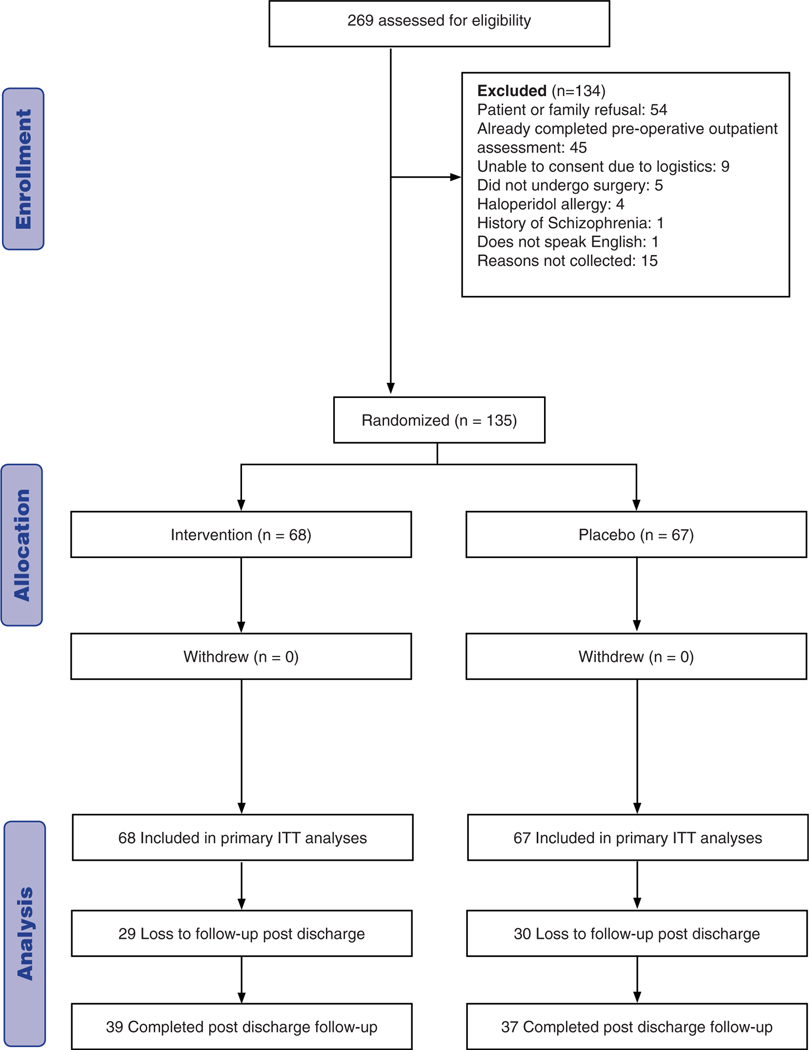
Participants: Individuals undergoing thoracic surgery (N=135).
Intervention: Low-dose intravenous haloperidol (0.5 mg three times daily for a total of 11 doses) administered postoperatively.
Measurements: The primary outcome was delirium incidence during hospitalization. Secondary outcomes were time to delirium, delirium duration, delirium severity, and ICU and hospital length of stay. Delirium was assessed using the Confusion Assessment Method for the ICU and delirium severity using the Delirium Rating Scale-Revised.
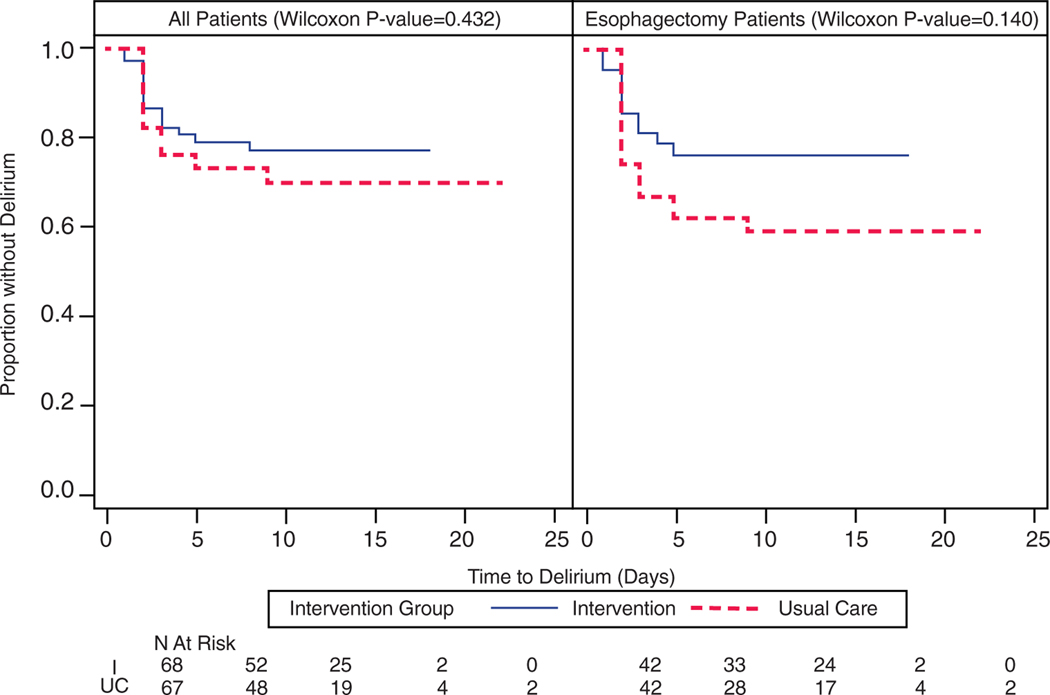
Results: Sixty-eight participants were randomized to receive haloperidol and 67 placebo. No significant differences were observed between those receiving haloperidol and those receiving placebo in incident delirium (n=15 (22.1%) vs n=19 (28.4%); p = .43), time to delirium (p = .43), delirium duration (median 1 day, interquartile range (IQR) 1-2 days vs median 1 day, IQR 1-2 days; p = .71), delirium severity, ICU length of stay (median 2.2 days, IQR 1-3.3 days vs median 2.3 days, IQR 1-4 days; p = .29), or hospital length of stay (median 10 days, IQR 8-11.5 days vs median 10 days, IQR 8-12 days; p = .41). In the esophagectomy subgroup (n = 84), the haloperidol group was less likely to experience incident delirium (n=10 (23.8%) vs n=17 (40.5%); p = .16). There were no differences in time to delirium (p = .14), delirium duration (median 1 day, IQR 1-2 days vs median 1 day, IQR 1-2 days; p = .71), delirium severity, or hospital length of stay (median 11 days, IQR 10-12 days vs median days 11, IQR 10-15 days; p = .26). ICU length of stay was significantly shorter in the haloperidol group (median 2.8 days, IQR 1.1-3.8 days vs median 3.1 days, IQR 2.1-5.1 days; p = .03). Safety events were comparable between the groups.
Conclusion: Low-dose postoperative haloperidol did not reduce delirium in individuals undergoing thoracic surgery but may be efficacious in those undergoing esophagectomy. J Am Geriatr Soc 66:2289-2297, 2018.
Trial registration: ClinicalTrials.gov NCT02213900.
Keywords: ICU; cognition; delirium; esophagectomy; haloperidol.
© 2018, Copyright the Authors Journal compilation © 2018, The American Geriatrics Society.
Conflict of interest statement
The study was supported by Indiana Health Values Fund Grant VFR 398 awarded to Dr. Babar Khan.
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Ed. Arlington, VA: American Psychiatric Publishing, 2013.
-
- Lin SM, Liu CY, Wang CH et al. The impact of delirium on the survival of mechanically ventilated patients. Crit Care Med 2004;32:2254–2259. - PubMed
-
- Jackson JC, Gordon SM, Hopkins RO et al. The association between delirium and cognitive decline: A review of the empirical literature. Neuropsychol Rev 2004;14:87–98. - PubMed
-
- Milbrandt EB, Deppen S, Harrison PL et al. Costs associated with delirium in mechanically ventilated patients. Crit Care Med 2004;32:955–962. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
