

Pediatric Anthracycline-Induced Cardiotoxicity: Mechanisms, Pharmacogenomics, and Pluripotent Stem-Cell Modeling
- PMID: 30460992
- PMCID: PMC6590110
- DOI: 10.1002/cpt.1311
Pediatric Anthracycline-Induced Cardiotoxicity: Mechanisms, Pharmacogenomics, and Pluripotent Stem-Cell Modeling
Abstract
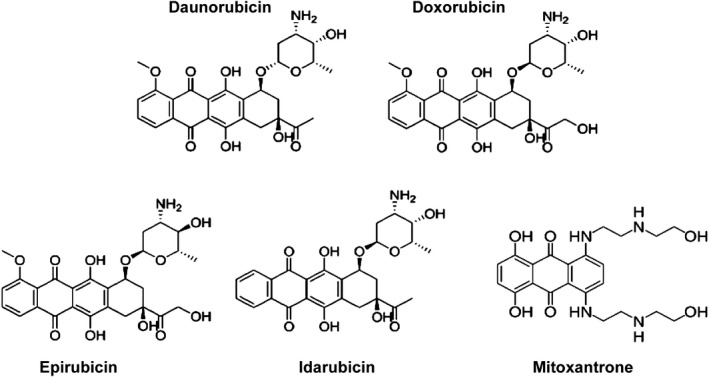
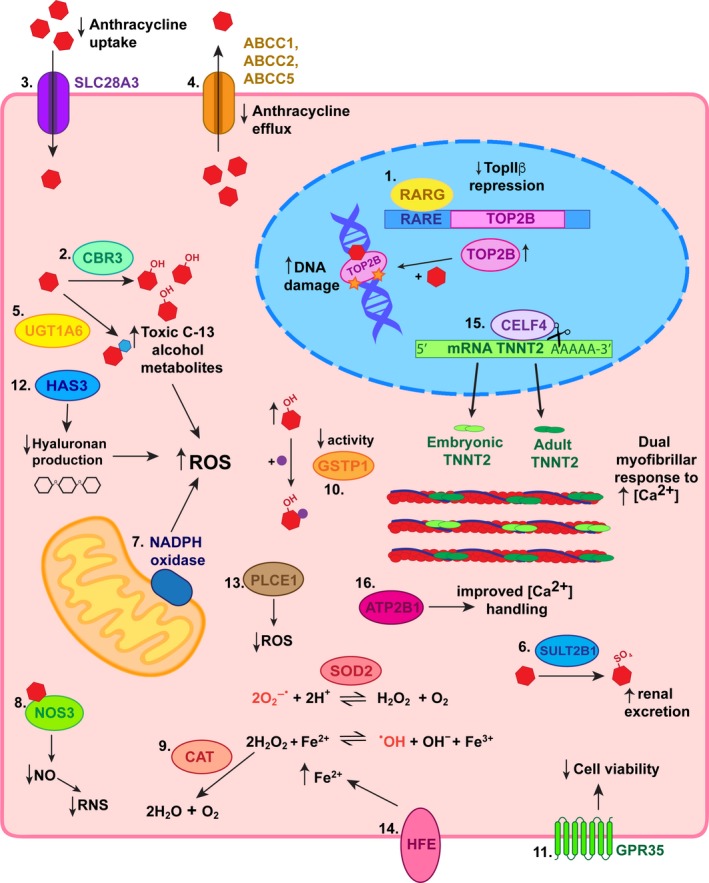
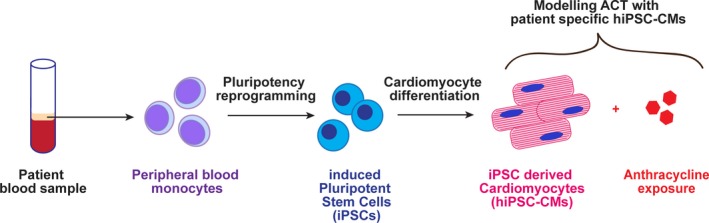
Anthracycline-induced cardiotoxicity (ACT) is a severe adverse drug reaction for a subset of children treated with anthracyclines as part of chemotherapy protocols. The identification of genetic markers associated with increased ACT susceptibility has clinical significance toward improving patient care and our understanding of the molecular mechanisms involved in ACT. Human-induced pluripotent stem cell-derived cardiomyocytes represent a novel approach to determine the pharmacogenomics of ACT and guide the development of genetic screening tests.
© 2018 Murdoch Childrens Research Institute. Clinical Pharmacology & Therapeutics published by Wiley Periodicals, Inc. on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures
References
-
- Miller, K. et al Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 66, 271–289 (2016). - PubMed
-
- Australian Childhood Cancer Registry . A summary of childhood cancer statistics 1983–2014. Queensland: Cancer Council (2014). <https://cancerqld.blob.core.windows.net/site/content/uploads/2017/12/A-s...>. Accessed February 27, 2018.
-
- Minotti, G. , Menna, P. , Salvatorelli, E. , Cairo, G. & Gianni, L. Anthracyclines: molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharmacol. Rev. 56, 185–229 (2004). - PubMed
-
- Jain, K. et al A prospective randomized comparison of epirubicin and doxorubicin in patients with advanced breast cancer. J. Clin. Oncol. 3, 818–826 (1985). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
