

Lymphomas diagnosed in an internal medicine department compared to lymphomas diagnosed in other departments: Clinical and outcome differences
- PMID: 30461623
- PMCID: PMC6392786
- DOI: 10.1097/MD.0000000000013228
Lymphomas diagnosed in an internal medicine department compared to lymphomas diagnosed in other departments: Clinical and outcome differences
Abstract
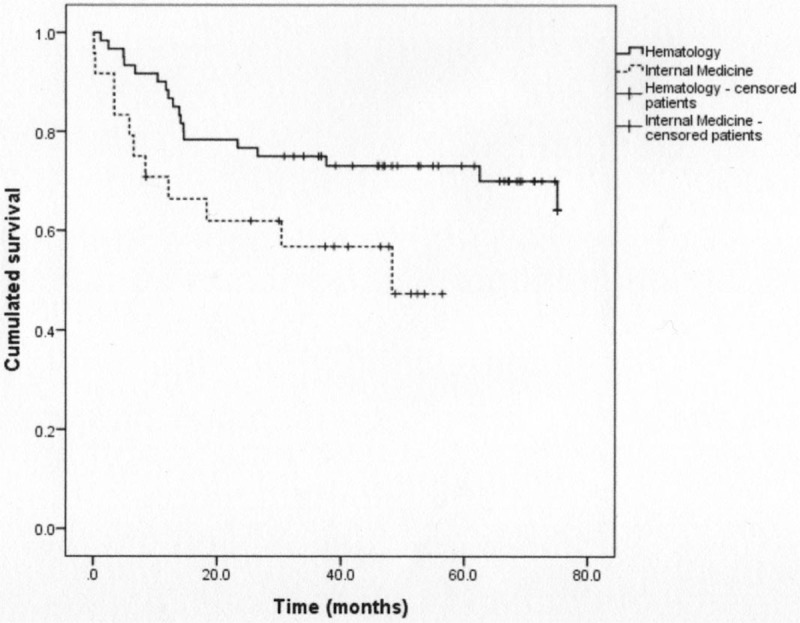
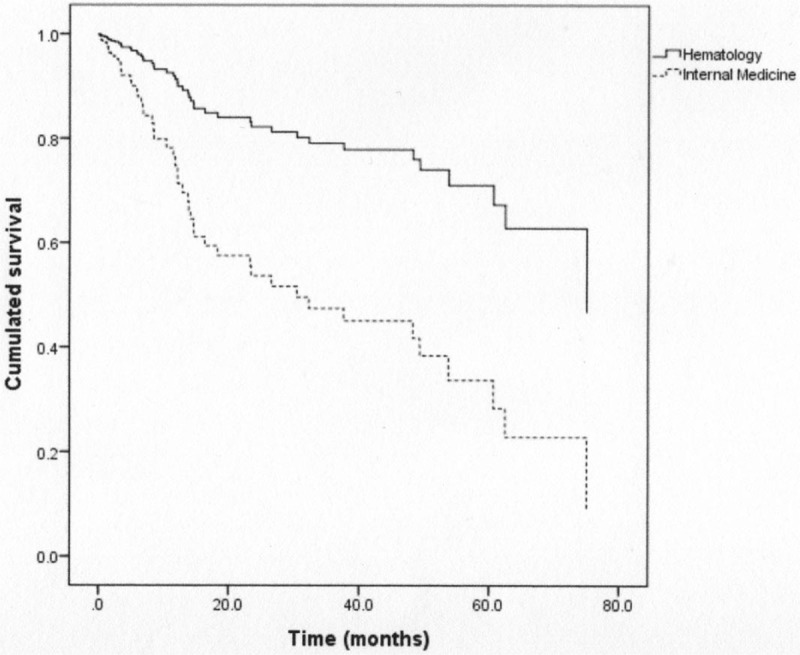
Lymphomas are common malignancies with highly variable clinical presentations and prognosis. Prognostic value of clinical presentation at onset is still questioned. The objective of this study was to compare the disease presentation and the outcome of lymphomas diagnosed in an Internal Medicine Department of a University Hospital to disease presentation and outcome of patients who were referred to the Hematology Department of the same institution by other departments or healthcare facilities.This retrospective monocentric observational study included 37 patients. They were matched to 73 patients, who were referred to the Hematology Department, according to age, histology, and Ann Arbor stage. The demographics, clinical and biological presentations, overall survival, and progression-free survival were compared.Patients diagnosed with lymphoma in the Internal Medicine Department were more likely to be febrile (67.5% vs 21.9%; P < .001) and have higher inflammatory markers (mean C-reactive protein 86.6 vs 56.3 mg/L; P = .02). The median overall survival of these patients was poorer (P < .001), even in the subset of patients treated with standard treatment, and remained shorter in multivariable analysis (P = .002). The specific treatment started earlier (20.2 vs 37.5 days; P = .006), but was more frequently palliative (37.8% vs 19.2%; P = .04). There was no significant difference in median progression-free survival.Lymphomas diagnosed in an Internal Medicine Department had aggressive clinical presentations and a poorer outcome, despite an early start of conventional treatment.
Figures
References
-
- A predictive model for aggressive non-Hodgkin's lymphoma. The International Non-Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med 1993; 329:987–994. - PubMed
-
- Hasenclever D, Diehl V. A prognostic score for advanced Hodgkin's disease. International Prognostic Factors Project on Advanced Hodgkin's Disease. N Engl J Med 1998;339:1506–14. - PubMed
-
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373–83. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
