

Comparison of Short-Term Clinical and Pathological Outcomes after Transanal versus Laparoscopic Total Mesorectal Excision for Low Anterior Rectal Resection Due to Rectal Cancer: A Systematic Review with Meta-Analysis
- PMID: 30463197
- PMCID: PMC6262322
- DOI: 10.3390/jcm7110448
Comparison of Short-Term Clinical and Pathological Outcomes after Transanal versus Laparoscopic Total Mesorectal Excision for Low Anterior Rectal Resection Due to Rectal Cancer: A Systematic Review with Meta-Analysis
Abstract
Background: Transanal total mesorectal excision (TaTME) is a new technique that is designed to overcome the limits of the open and laparoscopic approach for rectal resections.
Objective: This study is designed to compare TaTME with standard laparoscopic TME (LaTME).
Methods: We searched Medline, Embase, and Scopus databases covering a up to October 2018. Inclusion criteria for study enrolment: (1) study comparing laparoscopic resection of rectal cancer vs. TaTME for rectal malignancy, (2) reporting of overall morbidity, operative time, or major complications.
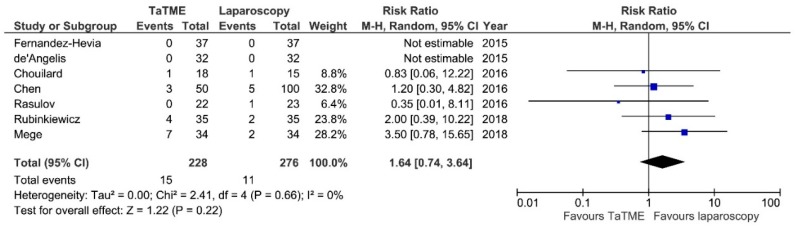
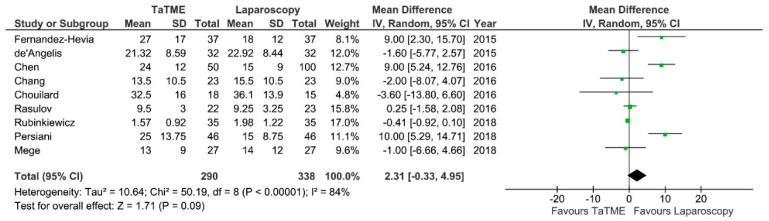
Results: Eleven non-randomized studies were eligible with a total of 778 patients. We found statistical significant differences in regard to major complications in favour of TaTME (RR = 0.55; 95% CI 0.31⁻0.97; p = 0.04). We did not found significant differences regarding overall complications intraoperative adverse effects, operative time, anastomotic leakage, intra-abdominal abscess occurrence, Surgical Site Infection, reoperations, Length of stay, completeness of mesorectal excision, R0 resection rate, number of harvested lymph nodes, circumferential resection margin, and distal resection margin.
Conclusions: This meta-analysis shows benefits of TaTME technique regarding major postoperative complications. Regarding clinicopathological features transanal approach is not superior to LaTME. Currently, the quality of the evidence on benefits of TaTME is low due to lack of randomized controlled trials, which needs to be taken into consideration in further evaluation of the technique. Further evaluation of TaTME require conducting large randomized control trials.
Keywords: laparoscopic; rectal cancer; total mesorectal excision; transanal.
Conflict of interest statement
The authors declare no conflict of interests.
Figures









References
-
- Pędziwiatr M., Małczak P., Mizera M., Witowski J., Torbicz G., Major P., Pisarska M., Wysocki M., Budzyński A. There is no difference in outcome between laparoscopic and open surgery for rectal cancer: A systematic review and meta-analysis on short- and long-term oncologic outcomes. Tech. Coloproctol. 2017;21:595–604. doi: 10.1007/s10151-017-1662-4. - DOI - PMC - PubMed
-
- Havenga K., Enker W.E., Norstein J., Moriya Y., Heald R.J., van Houwelingen H.C., van de Velde C.J. Improved survival and local control after total mesorectal excision or D3 lymphadenectomy in the treatment of primary rectal cancer: An international analysis of 1411 patients. Eur. J. Surg. Oncol. 1999;25:368–374. doi: 10.1053/ejso.1999.0659. - DOI - PubMed
LinkOut - more resources
Full Text Sources
