

Advanced Radiation Techniques in the Treatment of Esthesioneuroblastoma: A 7-Year Single-Institution's Clinical Experience
- PMID: 30463343
- PMCID: PMC6267306
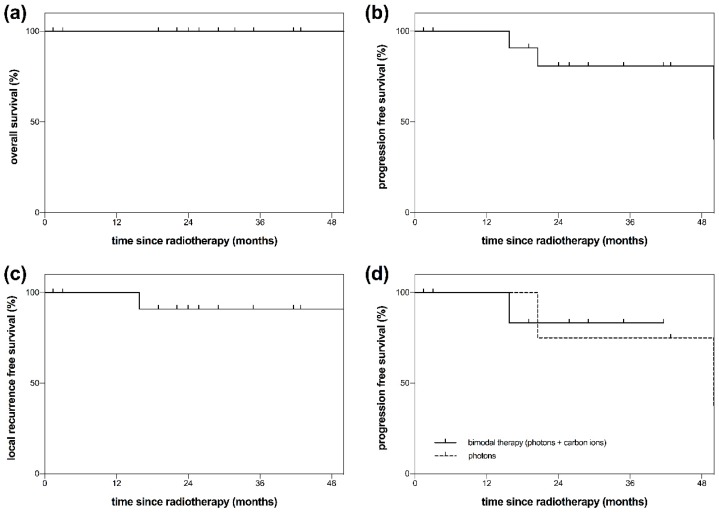
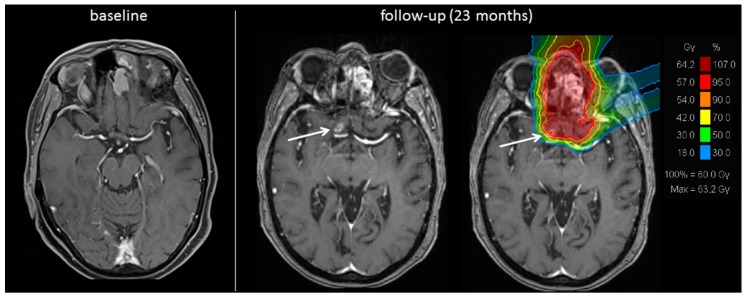
- DOI: 10.3390/cancers10110457
Advanced Radiation Techniques in the Treatment of Esthesioneuroblastoma: A 7-Year Single-Institution's Clinical Experience
Abstract
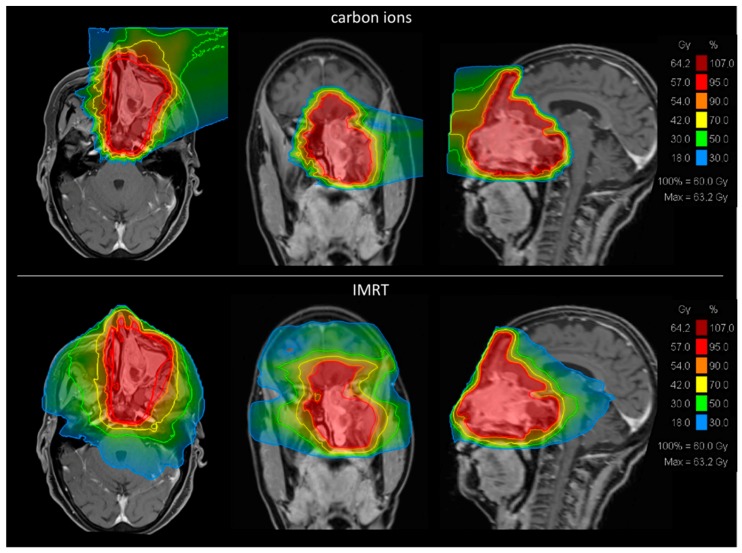
(1) Background: Esthesioneuroblastoma (ENB) is a rare tumor entity originating from the olfactory neuroepithelium. There is a scarcity of data about different treatment strategies. Intensity modulated radiotherapy (IMRT) and carbon ion radiotherapy (CIRT) are advanced radiation techniques that might improve local tumor control. (2) Methods: This retrospective analysis contained 17 patients with ENB (Kadish stage ≥ C: 88%; n = 15). Four patients had already undergone previous radiotherapy (RT). The treatment consisted of either IMRT (n = 5), CIRT (n = 4) or a combination of both techniques (n = 8). Median follow-up was 29 months. (3) Results: In patients that had not been irradiated before (n = 13), calculated overall survival (OS) and progression free survival (PFS) rates after 48 months were 100% and 81% respectively (Kaplan-Meier estimates). Two of four patients that underwent reirradiation died after RT, presumably due to tumor progression. Besides common toxicities, five patients (30%) showed mostly asymptomatic radiation-induced brain changes, most likely due to a disturbance of the blood-brain barrier. (4) Conclusions: Our results demonstrate that IMRT, CIRT, a combined approach of IMRT and CIRT as well as reirradiation with CIRT seem to be feasible and effective treatment methods in ENB.
Keywords: carbon ion radiation; esthesioneuroblastoma; olfactory neuroblastoma; particle therapy; radiotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Broich G., Pagliari A., Ottaviani F. Esthesioneuroblastoma: A general review of the cases published since the discovery of the tumour in 1924. Anticancer Res. 1997;17:2683–2706. - PubMed
-
- Association Française Pour L’étude du Cancer L’esthesioneuroepitheliome olfactif. Bulletin de l’Association Francaise pour l’etude du Cancer. 1924;13:410–421.
LinkOut - more resources
Full Text Sources
