

Menstrual and reproductive outcomes after use of balloon tamponade for severe postpartum hemorrhage
- PMID: 30463522
- PMCID: PMC6249747
- DOI: 10.1186/s12884-018-2085-6
Menstrual and reproductive outcomes after use of balloon tamponade for severe postpartum hemorrhage
Abstract
Background: The use of intrauterine balloon tamponade to manage postpartum hemorrhage is increasing. However, there is lack of studies on the menstrual and reproductive outcomes after such treatment. The purpose of this study is to explore the menstrual and reproductive outcomes for patients who had been managed by intrauterine balloon tamponade for severe postpartum hemorrhage in her index pregnancy.
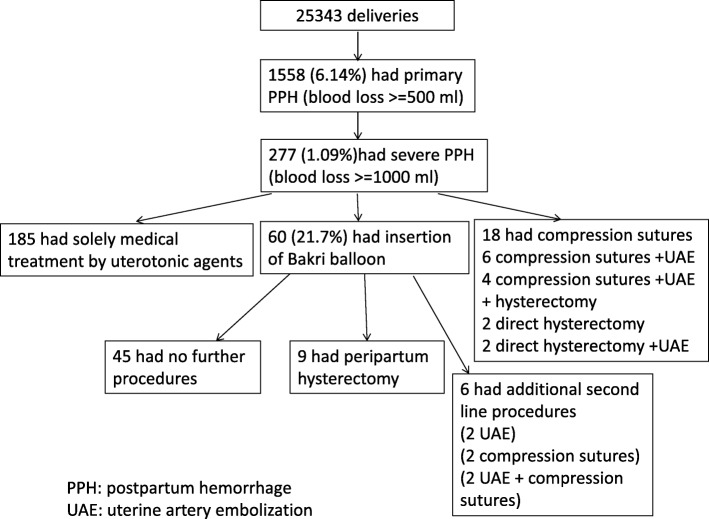
Methods: All patients who had delivered in United Christian Hospital from January 2011 to June 2016 with severe postpartum hemorrhage (PPH) (blood loss> = 1 L) were identified by the labour ward delivery registry and a comprehensive obstetric database. Patients who had intrauterine balloon tamponade inserted were compared with those managed solely by uterotonic agents as controls. Patients who had hysterectomy or additional procedures performed, such as compression sutures or uterine artery embolization were excluded from both groups. A questionnaire on menses, fertility and reproductive outcomes was mailed to both groups of patients. Those that had not replied within 4 weeks would receive a telephone survey.
Results: A total of 39 patients in the balloon tamponade group and 161 patients in the control group were recruited, which represented 87.0% of all eligible patients within the study period. The median follow up period was 45 months. All patients in the balloon tamponade group had return of menses after delivery. The majority of the patients (87.2%) in the balloon tamponade group had normal menstrual patterns in the 12 months after the index delivery as well as in the most recent 12 months. After excluding the patients with contraception, the subsequent pregnancy rate was 42.9% (9/21) in the balloon tamponade group compared to 45.9% (28/61) in the control group (p = 0.81). Among the 9 subsequent pregnancies in the balloon tamponade group, there were two miscarriages, one scar pregnancy, one induced abortion, while the remaining five were normal pregnancies with full term deliveries without intrauterine growth restriction. The majority of patients replied that they were satisfied with using Bakri balloon for PPH management in their index pregnancy.
Conclusions: Intrauterine balloon tamponade for the management of severe PPH appeared to pose little adverse effects on subsequent menstrual and reproductive function.
Keywords: Fertility; Intrauterine balloon tamponade; Menstruation; Postpartum hemorrhage; Pregnancy.
Conflict of interest statement
Author’s information
Kong CW, MBChB, MRCOG, FHKAM. Consultant of Department of O&G, United Christian Hospital, Hong Kong. Subspecialist in Maternal and Fetal Medicine.
Research interest on postpartum hemorrhage and balloon tamponade with a number of publications on this area.
To WWK, MBBS, MPH, M Phil, MD, FRCOG. Chief of Service, Department of O&G, United Christian Hospital, Hong Kong. Subspecialist in Maternal and Fetal Medicine. Had more than 50 publications on research in obstetrics.
Ethics approval and consent to participate
Ethics approval for this study was granted by the Kowloon Central/ Kowloon East Ethics Committee Board of the Hospital Authority, Hong Kong (KC/KE-16-0169/ER-1). Additional data was collected from the patients involved in the previous studies, for the current study. Consent was waived from the original studies, but written consent was obtained for the current study, and was attached to the questionnaire.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Knight M, Callaghan WM, Berg C, Alexander S, Bouvier-Colle MH, Ford JB, et al. Trends in postpartum hemorrhage in high resource countries: a review and recommendations from the international postpartum hemorrhage collaborative group. BMC Pregnancy Childbirth. 2009;9:55. doi: 10.1186/1471-2393-9-55. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
