

An intervention to control an ICU outbreak of carbapenem-resistant Acinetobacter baumannii: long-term impact for the ICU and hospital
- PMID: 30463589
- PMCID: PMC6249923
- DOI: 10.1186/s13054-018-2247-y
An intervention to control an ICU outbreak of carbapenem-resistant Acinetobacter baumannii: long-term impact for the ICU and hospital
Abstract
Background: Following a fatal intensive care unit (ICU) outbreak of carbapenem-resistant Acinetobacter baumanii (CRAB) in 2015, an aggressive infection control intervention was instituted. We outline the intervention and long-term changes in the incidence and prevalence of CRAB.
Methods: The infection control intervention included unit closure (3 days), environmental cleaning, hand hygiene interventions, and environmental culturing. CRAB acquisition and prevalence and colistin use were compared for the 1 year before and 2 years after the intervention.
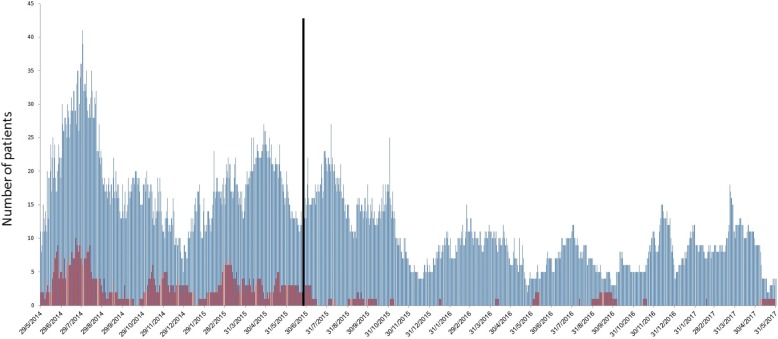
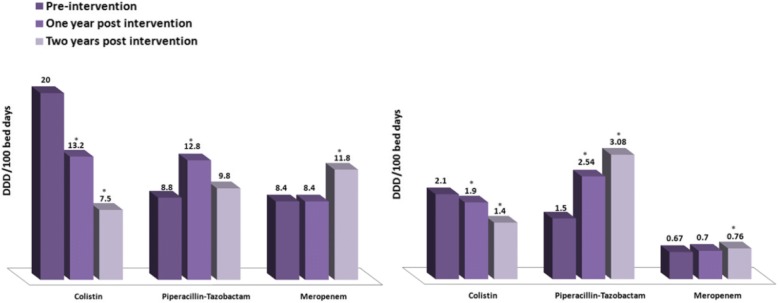
Results: Following the intervention, ICU CRAB acquisition decreased significantly from 54.6 (preintervention) to 1.9 (year 1) to 5.6 cases (year 2)/1000 admissions (p < 0.01 for comparisons with preintervention period.). Unexpectedly, ICU CRAB admission prevalence also decreased from 56.5 to 5.8 to 13 cases/1000 admissions (p < 0.001) despite the infection control intervention's being directed at the ICU alone. In parallel, hospital CRAB prevalence decreased from 4.4 to 2.4 to 2.5 cases/1000 admissions (p < 0.001), possibly as a result of decreased discharge of CRAB carriers from the ICU to the wards (58.5 to 1.9 to 7.4 cases/1000 admissions; p < 0.001). ICU colistin consumption decreased from 200 to 132 to 75 defined daily dose (DDD)/1000 patient-days (p < 0.05). Hospital colistin consumption decreased from 21.2 to 19.4 to 14.1 DDD/1000 patient-days (p < 0.05).
Conclusions: The ICU infection control intervention was highly effective, long-lasting, and associated with a decrease in last-line antibiotic use. The intervention was associated with the unexpected finding that hospital CRAB prevalence also decreased.
Keywords: Acinetobacter baumannii; ICU; Infection control; Outbreak.
Conflict of interest statement
Ethics approval and consent to participate
Information on ethics approval and consent is included in “Methods” section.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Kohlenberg A, Brummer S, Higgins PG, Sohr D, Piening BC, de Grahl C, Halle E, Ruden H, Seifert H. Outbreak of carbapenem-resistant Acinetobacter baumannii carrying the carbapenemase OXA-23 in a German university medical centre. J Med Microbiol. 2009;58(Pt 11):1499–1507. doi: 10.1099/jmm.0.012302-0. - DOI - PubMed
-
- Garlantezec R, Bourigault C, Boles JM, Prat G, Baron R, Tonnelier JM, Cosse M, Lefevre M, Jourdain S, Lelay G, et al. Cost-analysis of an intensive care unit closure due to an imipenem-resistant oxa-23 Acinetobacter baumannii outbreak. J Hosp Infect. 2011;77(2):174–175. doi: 10.1016/j.jhin.2010.09.027. - DOI - PubMed
-
- Ayraud-Thevenot S, Huart C, Mimoz O, Taouqi M, Laland C, Bousseau A, Castel O. Control of multi-drug-resistant Acinetobacter baumannii outbreaks in an intensive care unit: feasibility and economic impact of rapid unit closure. J Hosp Infect. 2012;82(4):290–292. doi: 10.1016/j.jhin.2012.08.016. - DOI - PubMed
-
- Molter G, Seifert H, Mandraka F, Kasper G, Weidmann B, Hornei B, Ohler M, Schwimmbeck P, Kroschel P, Higgins PG, et al. Outbreak of carbapenem-resistant Acinetobacter baumannii in the intensive care unit: a multi-level strategic management approach. J Hosp Infect. 2016;92(2):194–198. doi: 10.1016/j.jhin.2015.11.007. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
