

Iron deficiency diagnosed using hepcidin on critical care discharge is an independent risk factor for death and poor quality of life at one year: an observational prospective study on 1161 patients
- PMID: 30463596
- PMCID: PMC6249884
- DOI: 10.1186/s13054-018-2253-0
Iron deficiency diagnosed using hepcidin on critical care discharge is an independent risk factor for death and poor quality of life at one year: an observational prospective study on 1161 patients
Abstract
Background: Iron deficiency is difficult to diagnose in critically ill patients, but may be frequent and may impair recovery. Measurement of hepcidin could help in the diagnosis of iron deficiency. We aim to assess if iron deficiency diagnosed using hepcidin is associated with poorer outcome one year after an intensive care unit stay.
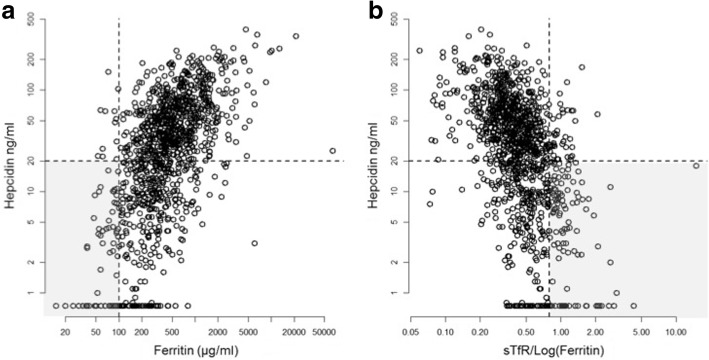
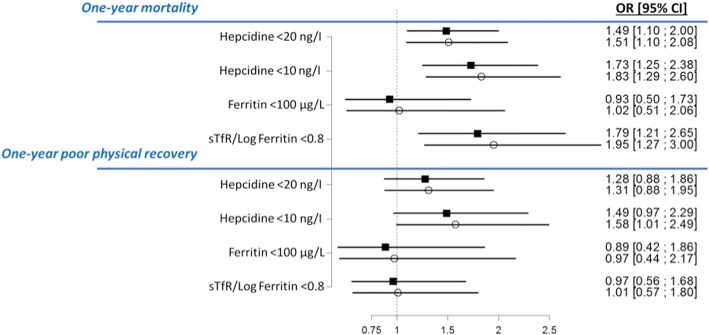
Methods: We used the prospective FROG-ICU, multicentre (n = 28 ICUs), observational cohort study of critically ill survivors followed up one year after intensive care unit discharge. Iron deficiency was defined as hepcidin < 20 ng/l, ferritin < 100 ng/l or soluble transferrin receptor (sTfR)/log(ferritin) > 0.8, measured in blood drawn at intensive care unit discharge. Main outcomes were one-year all-cause mortality and poor quality of life (defined as a Short Form 36 (SF-36) score below the median).
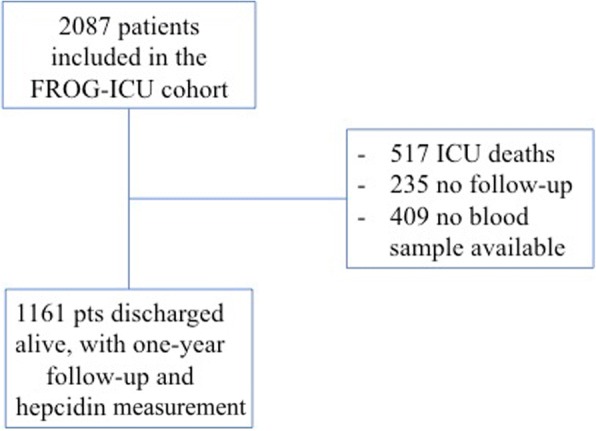
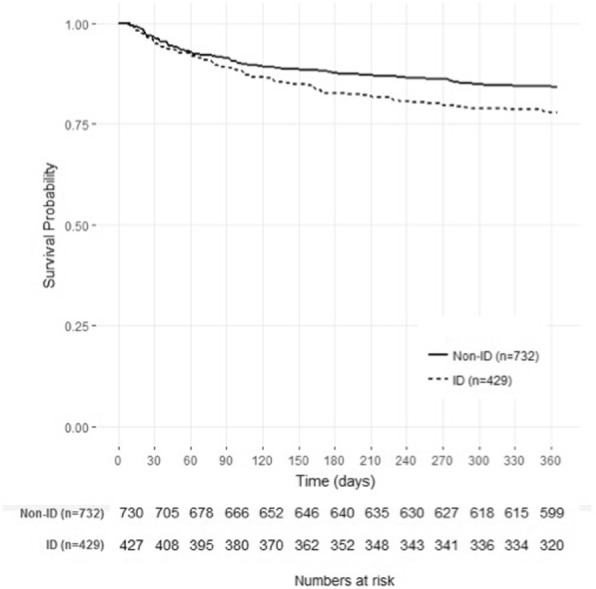
Results: Among the 2087 patients in the FROG-ICU cohort, 1570 were discharged alive and 1161 had a blood sample available at intensive care unit discharge and were included in the analysis. Using hepcidin, 429 (37%) patients had iron deficiency, compared to 72 (6%) using ferritin alone and 151 (13%) using the sTfR/log(ferritin) ratio. Iron deficiency diagnosed according to low hepcidin was an independent predictor of one-year mortality (OR 1.51 (1.10-2.08)) as was high sTfR/log ferritin ratio (OR = 1.95 (1.27-3.00)), but low ferritin was not. Severe ID, defined as hepcidin < 10 ng/l, was also an independent predictor of poor one-year physical recovery (1.58 (1.01-2.49)).
Conclusions: Iron deficiency, diagnosed using hepcidin, is very frequent at intensive care unit discharge and is associated with increased one-year mortality and poorer physical recovery. Whether iron treatment may improve these outcomes remains to be investigated.
Keywords: Critically ill; Hepcidin; Iron deficiency; Outcome; Quality of life.
Conflict of interest statement
Ethics approval and consent to participate
This study used data obtained from a previously published study, the FROG-ICU study [18, 19], conducted in France and Belgium in accordance with Good Clinical Practice (Declaration of Helsinki 2002) and Ethical Committee approvals (Comité de Protection des Personnes—Ile de France IV, IRB n° 00003835 and Commission d’éthique biomédicale hospitalo-facultaire de l’hôpital de Louvain, IRB n°B403201213352).
Consent for publication
Not applicable.
Competing interests
Sigismond Lasocki has received speaker honoraria from VIFOR Pharma, MASIMO, LFB and fees as a member of the advisory board and/or Steering Committee from VIFOR Pharma and Pfizer. AM received speaker’s honoraria from Abbott, Novartis, Orion, Roche and Servier, and fees as a member of the advisory board and/or Steering Committee from Cardiorentis, Adrenomed, MyCartis, Neurotronik and Sphyngotec. EG received a research grant from Sphingotec, and consultancy fees from Magnisense and Roche Diagnostics. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–1602. doi: 10.1016/S0140-6736(16)31678-6. - DOI - PMC - PubMed
-
- Jankowska EA, Rozentryt P, Witkowska A, Nowak J, Hartmann O, Ponikowska B, Borodulin-Nadzieja L, Banasiak W, Polonski L, Filippatos G, et al. Iron deficiency: an ominous sign in patients with systolic chronic heart failure. Eur Heart J. 2010;31(15):1872–1880. doi: 10.1093/eurheartj/ehq158. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
