

Overview of the pathological results and treatment characteristics in the first 1000 patients randomized in the SERC trial: axillary dissection versus no axillary dissection in patients with involved sentinel node
- PMID: 30463611
- PMCID: PMC6249981
- DOI: 10.1186/s12885-018-5053-7
Overview of the pathological results and treatment characteristics in the first 1000 patients randomized in the SERC trial: axillary dissection versus no axillary dissection in patients with involved sentinel node
Abstract
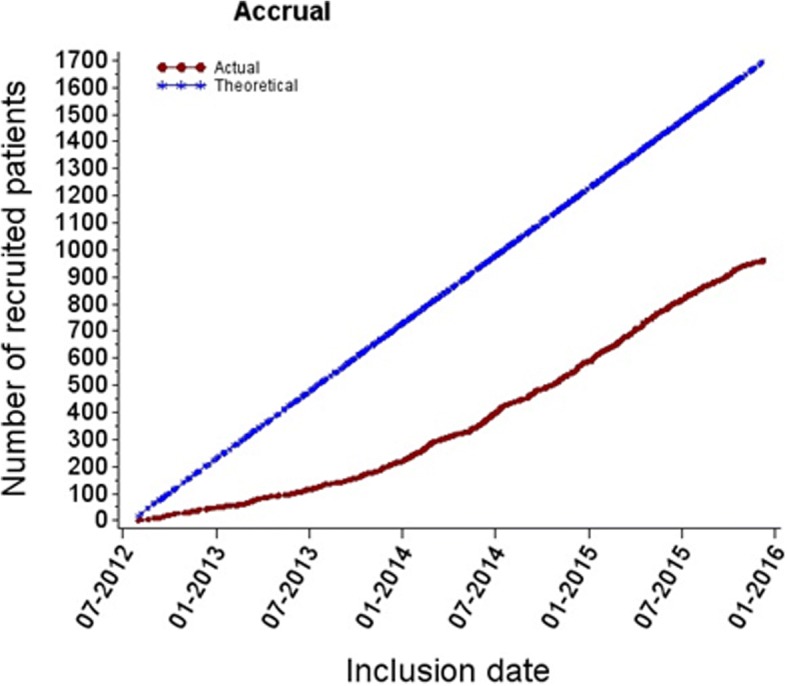
Background: Three randomized trials have concluded at non inferiority of omission of complementary axillary lymph node dissection (cALND) for patients with involved sentinel node (SN). However, we can outline strong limitations of these trials to validate this attitude with a high scientific level. We designed the SERC randomized trial ( ClinicalTrials.gov , number NCT01717131) to compare outcomes in patients with SN involvement treated with ALND or no further axillary treatment. The aim of this study was to analyze results of the first 1000 patients included.
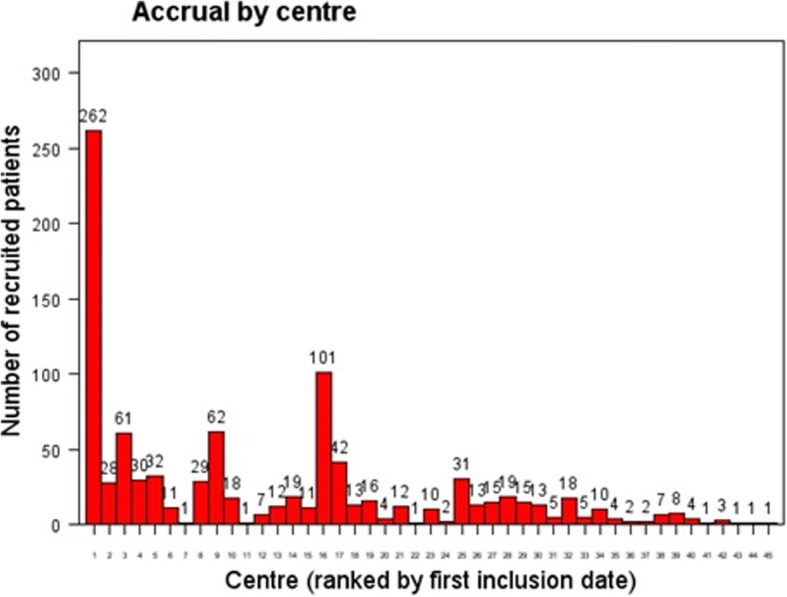
Methods: SERC trial is a multicenter non-inferiority phase 3 trial. Multivariate logistic regression analysis was used to identify independent factors associated with adjuvant chemotherapy administration and non-sentinel node (NSN) involvement.
Results: Of the 963 patients included in the analysis set, 478 were randomized to receive cALND and 485 SLNB alone. All patient demographics and tumor characteristics were balanced between the two arms. SN ITC was present in 6.3% patients (57/903), micro metastases in 33.0% (298), macro metastases in 60.7% (548) and 289 (34.2%) were non eligible to Z0011 trial criteria. Whole breast or chest wall irradiation was delivered in 95.9% (896/934) of patients, adjuvant chemotherapy in 69.5% (644/926), endocrine therapy in 89.6% (673/751) and the proportions were similar in the two arms. The overall rate of positive NSN was 19% (84/442) for patients with cALND. Crude rates of positive NSN according to SN status were 4.5% for ITC (1/22), 9.5% for micro metastases (13/137), 23.9% for macro metastases (61/255) and were respectively 29.36% (64/218), 9.33% (7/75) and 7.94% (10/126) when chemotherapy was administered after cALND, before cALND and for patients without chemotherapy.
Conclusion: The main objective of SERC trial is to demonstrate non inferiority of cALND omission. A strong interaction between timing of cALND and chemotherapy with positive NSN rate was observed.
Trial registration: This study is registered with ClinicalTrials.gov , number NCT01717131 October 19, 2012.
Keywords: Axillary lymph node dissection; Breast cancer; Randomized trial; Sentinel lymph node biopsy.
Conflict of interest statement
Ethics approval and consent to participate
All relevant ethical approvals from our institutional review board ethics committee (IPC - Comité d’Orientation Stratégique) have been obtained prior to study commencement.
Written informed consent was obtained from all patients prior to study entry.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Costantino JP, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11:927–933. doi: 10.1016/S1470-2045(10)70207-2. - DOI - PMC - PubMed
-
- Houvenaeghel G, Classe JM, Garbay JR, Giard S, Cohen M, Faure C, Charytansky H, Rouzier R, Daraï E, Hudry D, Azuar P, Villet R, Gimbergues P, Tunon de Lara C, Martino M, Fraisse J, Dravet F, Chauvet MP, Goncalves A, Lambaudie E. Survival impact and predictive factors of axillary recurrence after sentinel biopsy. Eur J Cancer. 2016;58:73–82. doi: 10.1016/j.ejca.2016.01.019. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
