

Impact of a Wearable Device-Based Walking Programs in Rural Older Adults on Physical Activity and Health Outcomes: Cohort Study
- PMID: 30463838
- PMCID: PMC6282012
- DOI: 10.2196/11335
Impact of a Wearable Device-Based Walking Programs in Rural Older Adults on Physical Activity and Health Outcomes: Cohort Study
Abstract
Background: Community-dwelling older adults living in rural areas are in a less favorable environment for health care compared with urban older adults. We believe that intermittent coaching through wearable devices can help optimize health care for older adults in medically limited environments.
Objective: We aimed to evaluate whether a wearable device and mobile-based intermittent coaching or self-management could increase physical activity and health outcomes of small groups of older adults in rural areas.
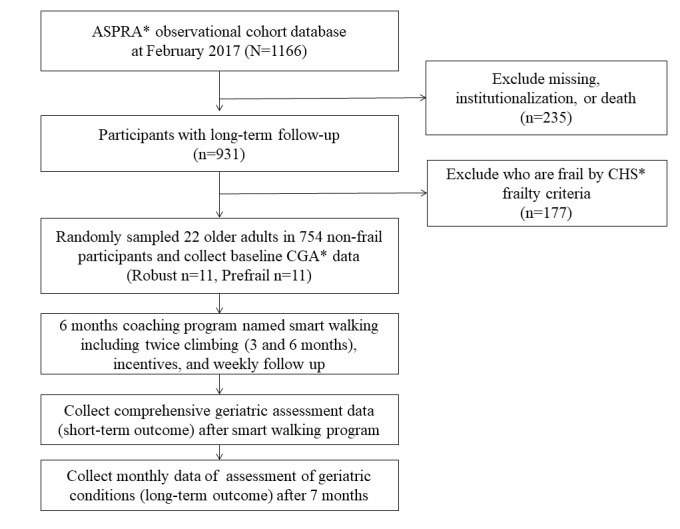
Methods: To address the above evaluation goal, we carried out the "Smart Walk" program, a health care model wherein a wearable device is used to promote self-exercise particularly among community-dwelling older adults managed by a community health center. We randomly selected older adults who had enrolled in a population-based, prospective cohort study of aging, the Aging Study of Pyeongchang Rural Area. The "Smart Walk" program was a 13-month program conducted from March 2017 to March 2018 and included 6 months of coaching, 1 month of rest, and 6 months of self-management. We evaluated differences in physical activity and health outcomes according to frailty status and conducted pre- and postanalyses of the Smart Walk program. We also performed intergroup analysis according to adherence of wearable devices.
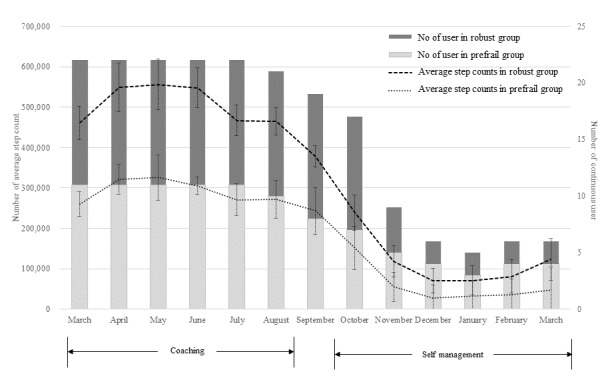
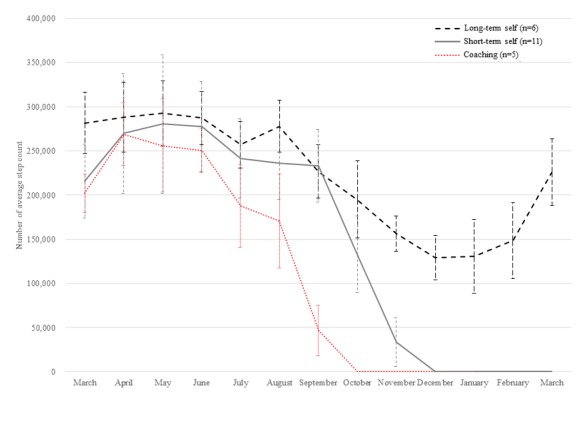
Results: We recruited 22 participants (11 robust and 11 prefrail older adults). The two groups were similar in most of the variables, except for age, frailty index, and Short Physical Performance Battery score associated with frailty criteria. After a 6-month coaching program, the prefrail group showed significant improvement in usual gait speed (mean 0.73 [SD 0.11] vs mean 0.96 [SD 0.27], P=.02), International Physical Activity Questionnaire scores in kcal (mean 2790.36 [SD 2224.62] vs mean 7589.72 [SD 4452.52], P=.01), and European Quality of Life-5 Dimensions score (mean 0.84 [SD 0.07] vs mean 0.90 [SD 0.07], P=.02), although no significant improvement was found in the robust group. The average total step count was significantly different and was approximately four times higher in the coaching period than in the self-management period (5,584,295.83 vs 1,289,084.66, P<.001). We found that participants in the "long-self" group who used the wearable device for the longest time showed increased body weight and body mass index by mean 0.65 (SD 1.317) and mean 0.097 (SD 0.513), respectively, compared with the other groups.
Conclusions: Our "Smart Walk" program improved physical fitness, anthropometric measurements, and geriatric assessment categories in a small group of older adults in rural areas with limited resources for monitoring. Further validation through various rural public health centers and in a large number of rural older adults is required.
Keywords: adherence; frailty; older adult; rural area; wearable device.
©Il-Young Jang, Hae Reong Kim, Eunju Lee, Hee-Won Jung, Hyelim Park, Seon-Hee Cheon, Young Soo Lee, Yu Rang Park. Originally published in JMIR Mhealth and Uhealth (http://mhealth.jmir.org), 21.11.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Jung YJ, Yoon JL, Kim HS, Lee A-Y, Kim MY, Cho JJ. Atypical Clinical Presentation of Geriatric Syndrome in Elderly Patients With Pneumonia or Coronary Artery Disease. Ann Geriatr Med Res. 2017 Dec 31;21(4):158–163. doi: 10.4235/agmr.2017.21.4.158. - DOI
-
- Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013 Mar 02;381(9868):752–62. doi: 10.1016/S0140-6736(12)62167-9. http://europepmc.org/abstract/MED/23395245 - DOI - PMC - PubMed
-
- Puts MTE, Toubasi S, Andrew MK, Ashe MC, Ploeg J, Atkinson E, Ayala AP, Roy A, Rodríguez Monforte Miriam, Bergman H, McGilton K. Interventions to prevent or reduce the level of frailty in community-dwelling older adults: a scoping review of the literature and international policies. Age Ageing. 2017 May 01;46(3):383–392. doi: 10.1093/ageing/afw247. http://europepmc.org/abstract/MED/28064173 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
