

GM-CSF inhibition reduces cytokine release syndrome and neuroinflammation but enhances CAR-T cell function in xenografts
- PMID: 30463995
- PMCID: PMC6376281
- DOI: 10.1182/blood-2018-10-881722
GM-CSF inhibition reduces cytokine release syndrome and neuroinflammation but enhances CAR-T cell function in xenografts
Abstract
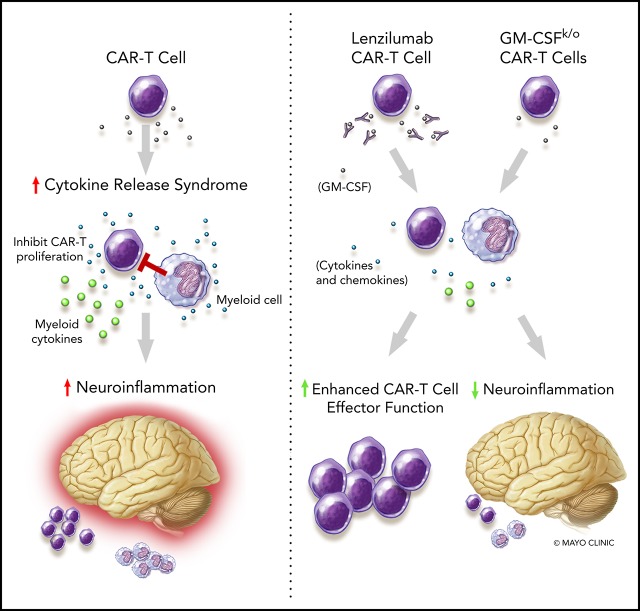
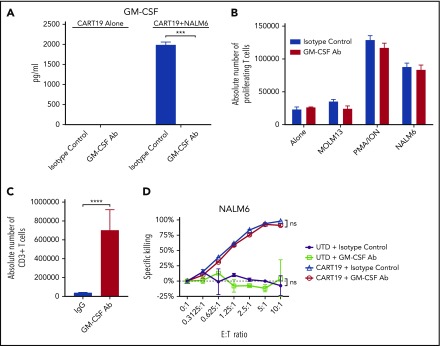
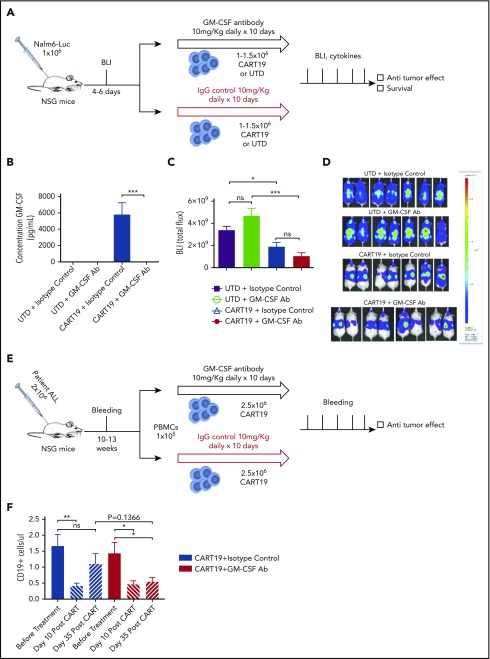
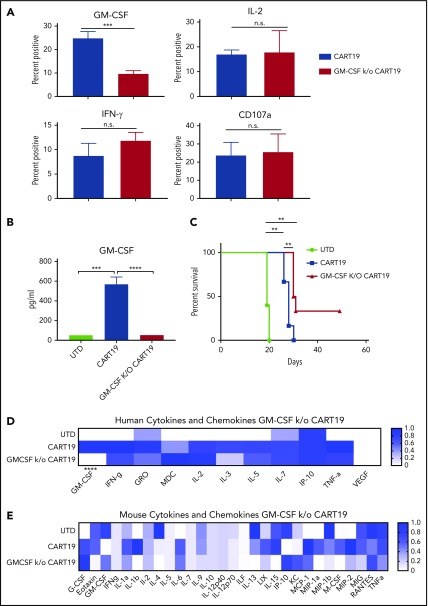
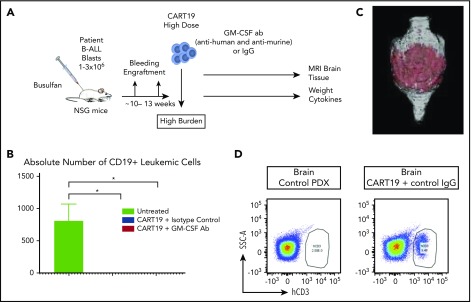
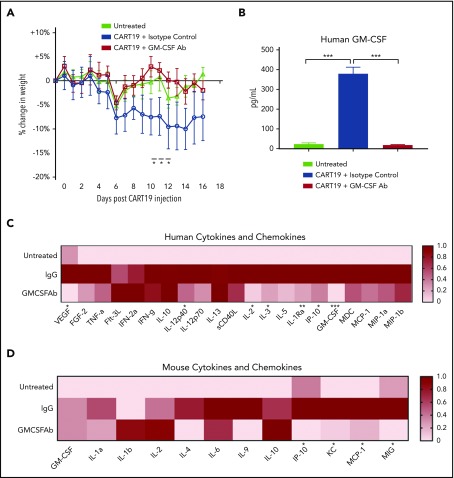
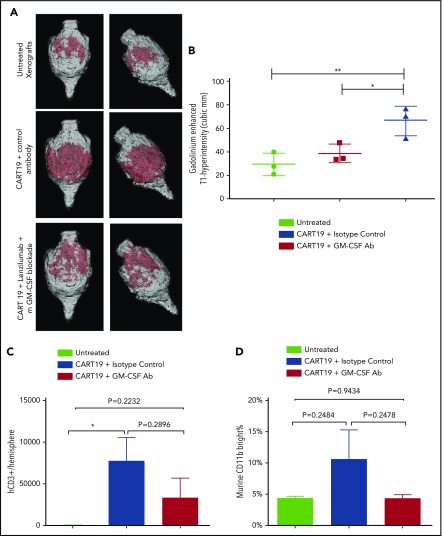
Chimeric antigen receptor T (CAR-T) cell therapy is a new pillar in cancer therapeutics; however, its application is limited by the associated toxicities. These include cytokine release syndrome (CRS) and neurotoxicity. Although the IL-6R antagonist tocilizumab is approved for treatment of CRS, there is no approved treatment of neurotoxicity associated with CD19-targeted CAR-T (CART19) cell therapy. Recent data suggest that monocytes and macrophages contribute to the development of CRS and neurotoxicity after CAR-T cell therapy. Therefore, we investigated neutralizing granulocyte-macrophage colony-stimulating factor (GM-CSF) as a potential strategy to manage CART19 cell-associated toxicities. In this study, we show that GM-CSF neutralization with lenzilumab does not inhibit CART19 cell function in vitro or in vivo. Moreover, CART19 cell proliferation was enhanced and durable control of leukemic disease was maintained better in patient-derived xenografts after GM-CSF neutralization with lenzilumab. In a patient acute lymphoblastic leukemia xenograft model of CRS and neuroinflammation (NI), GM-CSF neutralization resulted in a reduction of myeloid and T cell infiltration in the central nervous system and a significant reduction in NI and prevention of CRS. Finally, we generated GM-CSF-deficient CART19 cells through CRISPR/Cas9 disruption of GM-CSF during CAR-T cell manufacturing. These GM-CSFk/o CAR-T cells maintained normal functions and had enhanced antitumor activity in vivo, as well as improved overall survival, compared with CART19 cells. Together, these studies illuminate a novel approach to abrogate NI and CRS through GM-CSF neutralization, which may potentially enhance CAR-T cell function. Phase 2 studies with lenzilumab in combination with CART19 cell therapy are planned.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: S.S.K. is an inventor on patents in the field of CAR-T cell therapy that are licensed to Novartis (under an agreement among the Mayo Clinic, the University of Pennsylvania, and Novartis). O.A., T.S., D.C., and C.D. are employed by Humanigen. R.M.S., R.S., M.J.C., and S.S.K. are inventors on patents related to this work. The remaining authors declare no competing financial interests.
Figures
References
-
- Kenderian SS, Ruella M, Gill S, Kalos M. Chimeric antigen receptor T-cell therapy to target hematologic malignancies. Cancer Res. 2014;74(22):6383-6389. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
