

Retrospective comparative analysis of risk factors and outcomes in patients with carbapenem-resistant Acinetobacter baumannii bloodstream infections: cefoperazone-sulbactam associated with resistance and tigecycline increased the mortality
- PMID: 30464544
- PMCID: PMC6208797
- DOI: 10.2147/IDR.S169432
Retrospective comparative analysis of risk factors and outcomes in patients with carbapenem-resistant Acinetobacter baumannii bloodstream infections: cefoperazone-sulbactam associated with resistance and tigecycline increased the mortality
Abstract
Background: Carbapenem-resistant Acinetobacter baumannii (CRAB) is a rapidly emerging, life-threatening nosocomial infection. This study aimed to explore the risk factors, clinical features, antimicrobial therapy, and outcomes of CRAB bloodstream infections (BSIs).
Methods: This is a retrospective, comparative analysis of data from patients with A. baumannii BSI, treated from 2012 to 2015 at a tertiary teaching hospital. Risk factors associated with CRAB BSI and factors associated with the 28-day mortality were evaluated using logistic analyses.
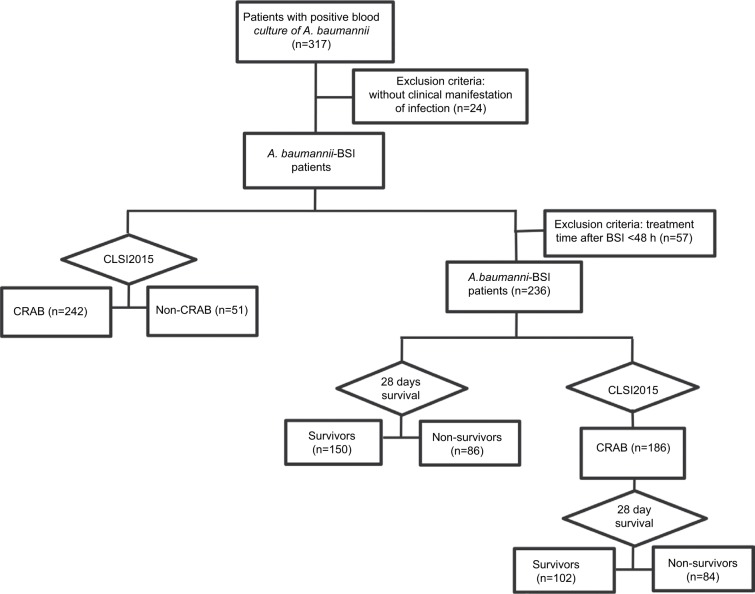
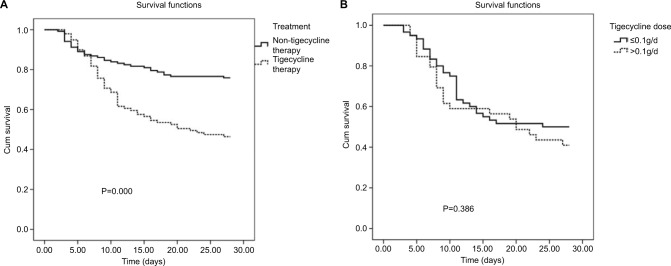
Results: Data from 293 patients with confirmed A. baumannii BSI were included; 242 (82.6%) patients had CRAB BSI and 51 (17.4%) patients had non-CRAB BSI. Risk factors significantly associated with CRAB BSI were a previous intensive care unit (ICU) stay (P=0.029), cefoperazone-sulbactam use (P=0.030), and carbapenem use (P=0.004). Among 236 patients with A. baumannii BSI who were evaluable at 28 days after receiving antibacterial therapy, there were 86 deaths. Factors associated with the 28-day mortality were ICU stay after BSI (P=0.040), readmission within 90 days (P=0.029), Acute Physiology and Chronic Health Evaluation II (APACHE II) score at diagnosis >19 (P=0.012), tigecycline therapy (P=0.021), presence of septic shock (P=0.029), and multiple organ failure (P=0.016). Death rates in patients treated with tigecycline were 53.5% vs 24.1% in patients treated with other agents. Among 186 patients with CRAB BSI evaluable at 28 days, 84 patients died. The associated risk factors were an ICU stay after BSI (P=0.036), APACHE II score >19 at diagnosis (P = 0.002), presence of septic shock (P=0.030), and multiple organ failure (P=0.007).
Conclusion: This study demonstrated that an ICU stay and cefoperazone-sulbactam or carbapenem use were seen to be the risk factors associated with the development of CRAB BSI. Critical illness and tigecycline therapy were significantly associated with higher mortality of patients with A. baumannii BSI.
Keywords: Acinetobacter baumannii; bloodstream infection; carbapenem-resistant; cefoperazone-sulbactam; tigecycline.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Higgins PG, Dammhayn C, Hackel M, Seifert H. Global spread of carbapenem-resistant Acinetobacter baumannii. J Antimicrob Chemother. 2010;65(2):233–238. - PubMed
-
- Boucher HW, Talbot GH, Bradley JS, et al. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin Infect Dis. 2009;48(1):1–12. - PubMed
-
- Karageorgopoulos DE, Falagas ME. Current control and treatment of multidrug-resistant Acinetobacter baumannii infections. Lancet Infect Dis. 2008;8(12):751–762. - PubMed
-
- Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–2329. - PubMed
-
- Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39(3):309–317. - PubMed
LinkOut - more resources
Full Text Sources
