

Epidural dexmedetomidine infusion for perioperative analgesia in patients undergoing abdominal cancer surgery: randomized trial
- PMID: 30464585
- PMCID: PMC6214321
- DOI: 10.2147/JPR.S163975
Epidural dexmedetomidine infusion for perioperative analgesia in patients undergoing abdominal cancer surgery: randomized trial
Abstract
Objective: To assess the postoperative analgesic efficacy of epidural dexmedetomidine added to bupivacaine infusion for patients undergoing major abdominal cancer surgery.
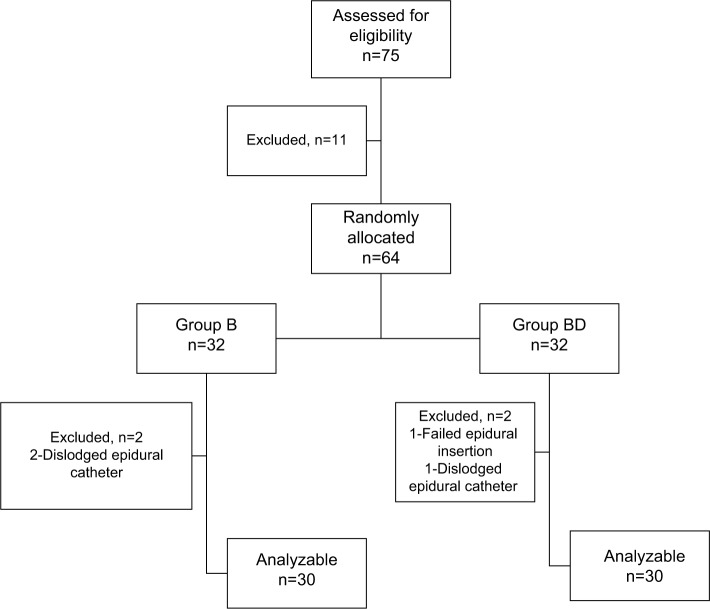
Methods: Patients scheduled for major upper abdominal cancer surgery were allocated to group bupivacaine (n =32), in which patients received epidural bupivacaine infusion (6 mL/h bupivacaine 0.1%) for 48 hours postoperatively, or group bupivacaine + dexmedetomidine (n=32), in which patients received epidural dexmedetomidine added to bupivacaine infusion (6 mL/h of bupivacaine 0.1% + dexmedetomidine, 0.5 µg/mL) for 48 hours postoperatively. The cumulative morphine consumption, the time to first analgesic request, and the VAS pain score were evaluated.
Results: The cumulative morphine consumption was significantly reduced in group bupivacaine + dexmedetomidine compared with group bupivacaine: mean ± SD of 10.40±5.16 mg vs 23.23±8.37 mg with an estimated difference (95% CI) of -12.83 (-16.43, -9.24), (P<0.001). The time to the first analgesic demand was significantly delayed in group bupivacaine + dexmedetomidine compared with group bupivacaine: median (IQR) of 6 (1.75, 8.25) h vs 1 (0, 4)h, (P<0.001). The mean collapsed over time of overall VAS pain scores at rest and movement was significantly reduced in group bupivacaine + dexmedetomidine compared with group bupivacaine : mean ± SE of 1.6±0.08 vs 2.38±0.08 with an estimated difference (95% CI) of -0.8 (-1, -0.86), (P<0.001), and mean ± SE of 2.17±0.07 vs 3.25±0.07 with an estimated difference (95% CI) of -1.1 (-1.27, - 0.89), (P<0.001), respectively.
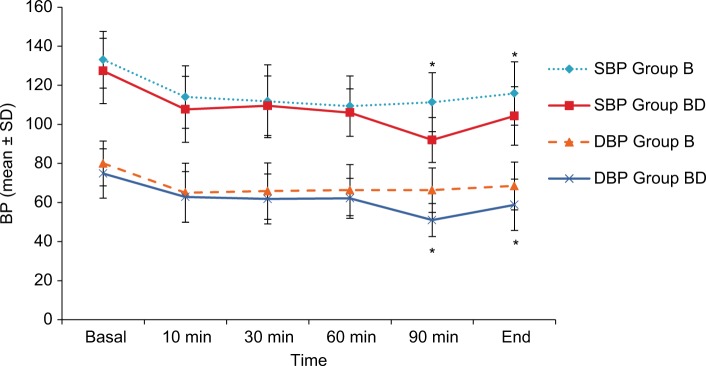
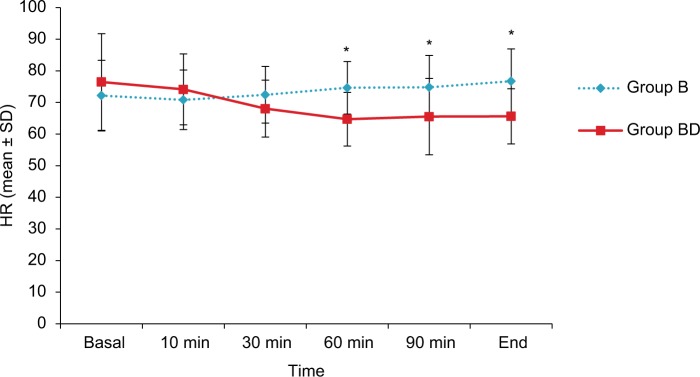
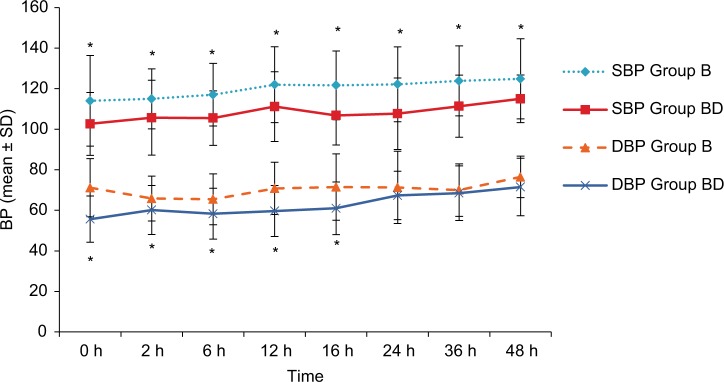
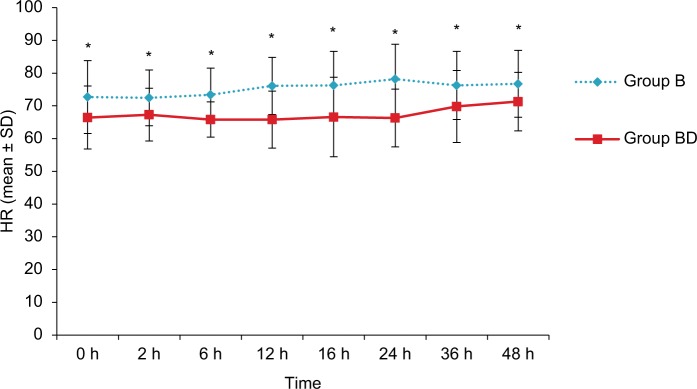
Conclusion: Epidural infusion of dexmedetomidine added to bupivacaine for patients undergoing major abdominal cancer surgery significantly reduced morphine consumption, delayed time to first analgesic supplementation, and decreased pain intensity during the first 48 hours postoperatively without harmful derangement on hemodynamics.
Keywords: dexmedetomidine; epidural; postoperative pain.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Werawatganon T, Charuluxanun S. Patient controlled intravenous opioid analgesia versus continuous epidural analgesia for pain after intra-abdominal surgery. Cochrane Database Syst Rev. 2005;1(1):CD004088. - PubMed
-
- Hjortsø NC, Lund C, Mogensen T, Bigler D, Kehlet H. Epidural morphine improves pain relief and maintains sensory analgesia during continuous epidural bupivacaine after abdominal surgery. Anesth Analg. 1986;65(10):1033–1036. - PubMed
-
- Gordh T. Epidural clonidine for treatment of postoperative pain after thoracotomy. A double-blind placebo-controlled study. Acta Anaesthesiol Scand. 1988;32(8):702–709. - PubMed
-
- Subramaniam B, Subramaniam K, Pawar DK, Sennaraj B. Preoperative epidural ketamine in combination with morphine does not have a clinically relevant intra- and postoperative opioid-sparing effect. Anesth Analg. 2001;93(5):1321–1326. - PubMed
LinkOut - more resources
Full Text Sources
Medical
