

Coronary CTA for Surveillance of Cardiac Allograft Vasculopathy
- PMID: 30464783
- PMCID: PMC6223999
- DOI: 10.1007/s12410-018-9467-z
Coronary CTA for Surveillance of Cardiac Allograft Vasculopathy
Erratum in
-
Correction to: Coronary CTA for Surveillance of Cardiac Allograft Vasculopathy.Curr Cardiovasc Imaging Rep. 2019;12(1):1. doi: 10.1007/s12410-018-9476-y. Epub 2018 Nov 8. Curr Cardiovasc Imaging Rep. 2019. PMID: 31186826 Free PMC article.
Abstract
Purpose of review: The purpose of this review is to highlight recent hardware and software advances in coronary computed tomography angiography (CTA) that make it a potentially viable alternative to invasive coronary angiography for surveillance of cardiac allograft vasculopathy (CAV) in heart transplant recipients.
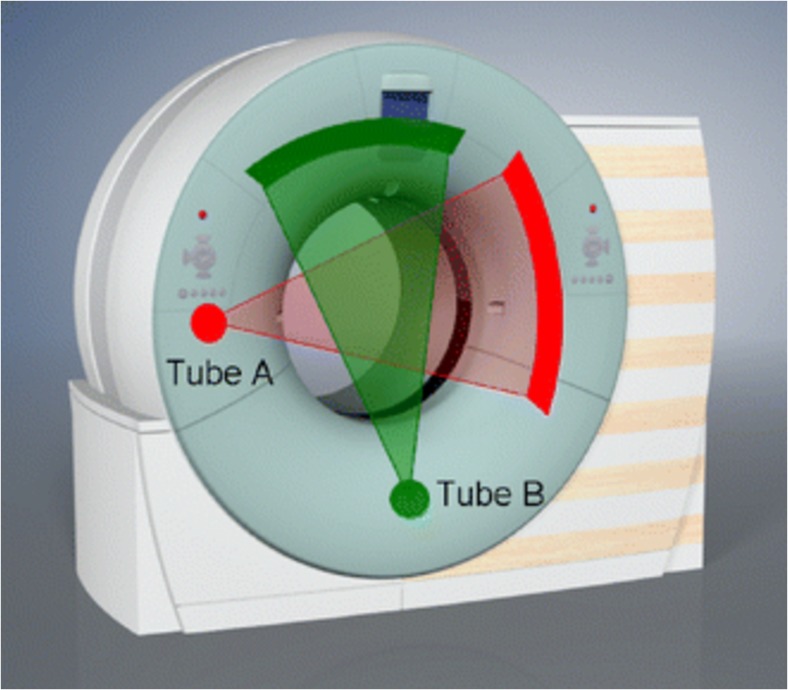
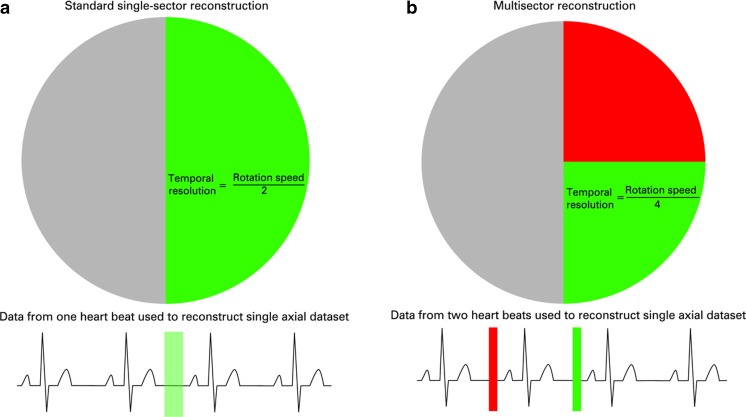
Recent findings: Dual-source CT, multisegment reconstruction, and intracycle motion correction algorithms are all technologies applied during or after image acquisition that can improve image quality and diagnostic accuracy in patients with elevated heart rates, such as heart transplant recipients. CT fractional flow reserve may also add value in this clinical scenario.
Summary: Coronary CTA now has equivalent diagnostic accuracy, offers more nuanced anatomic information, is inherently safer, and could be less costly than invasive coronary angiography. For these reasons, coronary CTA may now be a viable alternative to ICA for CAV surveillance in heart transplant recipients.
Keywords: Cardiac allograft vasculopathy; Coronary CT angiography; Dual-source CT; Intracycle motion correction; Multisegment reconstruction.
Conflict of interest statement
The opinions and assertions herein are those of the authors alone and do not represent the views of the U.S. Army, Office of the Surgeon General, Department of Defense, or the US Government. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures




References
-
- Lund LH, Khush KK, Cherikh WS, et al. The Registry of the International Society for Heart and Lung Transplantation: thirty-fourth adult heart transplantation report-2017; focus theme: allograft ischemic time. J Heart Lung Transplant. 2017;36:1037–1046. doi: 10.1016/j.healun.2017.07.019. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous