

Treatment Persistence and Healthcare Costs Among Patients with Rheumatoid Arthritis After a Change in Targeted Therapy
- PMID: 30464787
- PMCID: PMC6207310
Treatment Persistence and Healthcare Costs Among Patients with Rheumatoid Arthritis After a Change in Targeted Therapy
Abstract
Background: Targeted disease-modifying antirheumatic drug (DMARD) options for rheumatoid arthritis (RA) include tumor necrosis factor (TNF) inhibitors (adalimumab, certolizumab, etanercept, golimumab, infliximab) or alternative mechanisms of action (MOAs), such as a T-cell co-stimulation modulator (abatacept), Janus kinase inhibitor (tofacitinib), or interleukin-6 inhibitor (tocilizumab).
Objective: To examine treatment persistence and healthcare costs in patients with RA who changed therapy by cycling therapy (ie, switching within the same drug class), or switching between, the TNF inhibitors and alternative MOA medication classes.
Methods: We analyzed medical and pharmacy claims for commercially insured patients who cycled or switched between targeted DMARD agents between January 1, 2010, and September 30, 2014 (ie, the index date), to determine treatment patterns (ie, treatment switching, discontinuation, restarting after a gap ≥60 days, or persistence) and costs (plan- and patient-paid) for 1 year postindex. The cost per persistent patient was the total healthcare cost divided by the number of treatment-persistent patients.
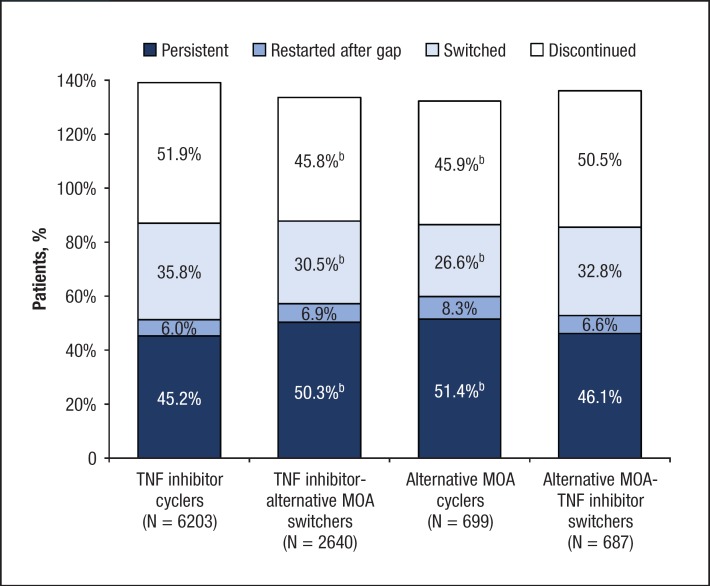
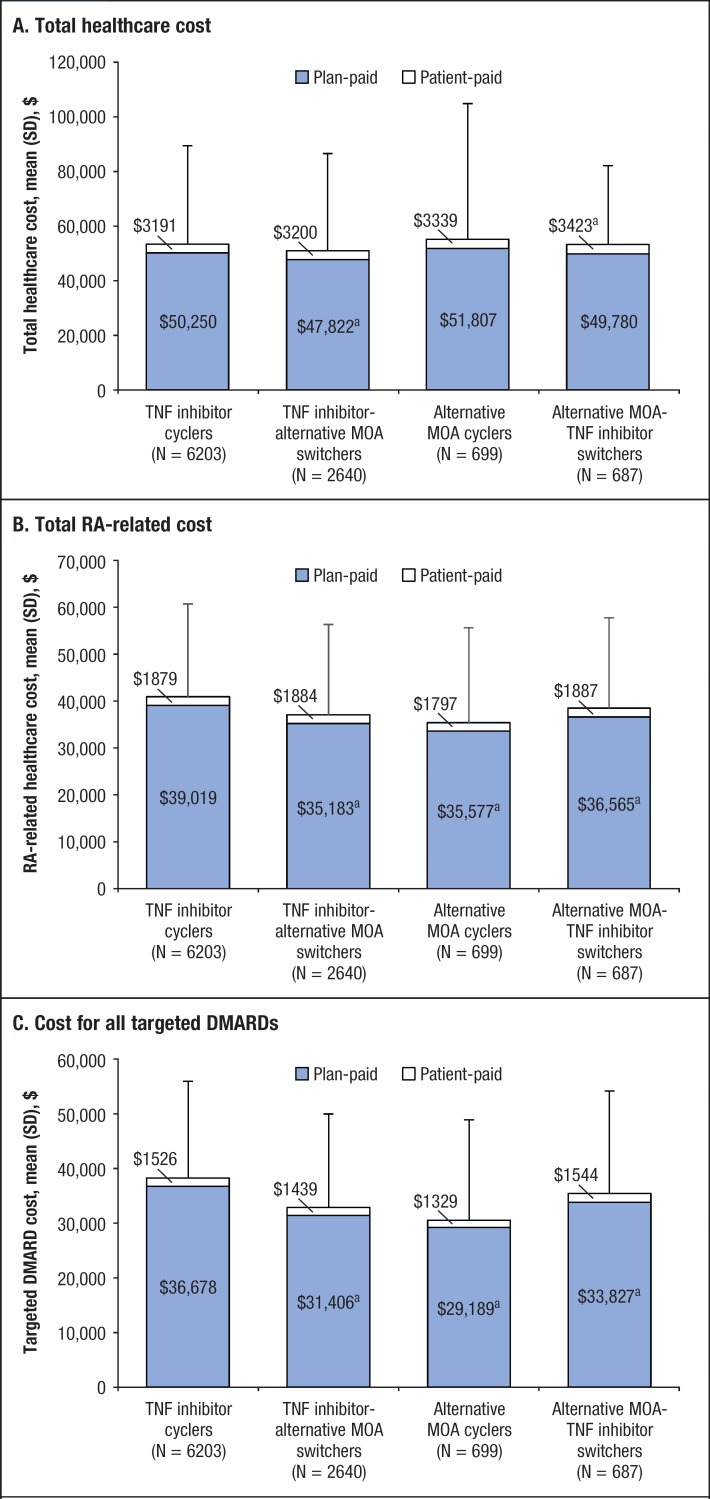
Results: The analysis included 6203 patients who cycled between TNF inhibitors, 2640 patients who switched from TNF inhibitors to alternative MOA agents, 699 patients who cycled between alternative MOA agents, and 687 patients who switched from alternative MOA agents to TNF inhibitors. The 1-year treatment persistence rates (with P values vs TNF inhibitor cyclers) were 45.2% for TNF inhibitor cyclers, 50.3% for TNF inhibitor-alternative MOA switchers (P <.001), 51.4% for alternative MOA agent cyclers (P = .002), and 46.1% for alternative MOA-TNF inhibitor switchers (P = .63). Compared with TNF inhibitor cyclers, the cost per persistent patient was lower for TNF inhibitor-alternative MOA switchers (-$16,853 RA-related; -$19,280 targeted DMARDs), alternative MOA agent cyclers (-$21,662 RA-related; -$25,153 targeted DMARDs), and alternative MOA-TNF inhibitor cyclers (-$7206 RA-related; -$7919 targeted DMARDs).
Conclusion: Among patients with RA, patients who switched from a TNF inhibitor to an alternative MOA agent and those who cycled between alternative MOA agents had significantly higher treatment persistence rates and a substantially lower cost per persistent patient than those who cycled between TNF inhibitors. These findings support the evaluation of switching medication classes for patients with RA when a targeted therapy fails.
Keywords: alternative mechanisms of action; cost; persistence; rheumatoid arthritis; switching treatment; synthetic DMARD; treatment cycling; treatment persistence; tumor necrosis factor inhibitors.
Figures
References
-
- Singh JA, Saag KG, Bridges SL, Jr, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68:1–26. - PubMed
-
- Smolen JS, Landewé R, Bijlsma J, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76:960–977. - PubMed
-
- Saag KG, Teng GG, Patkar NM, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59:762–784. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous