

Feasibility of a musculoskeletal ultrasound intervention to improve adherence in juvenile idiopathic arthritis: a proof-of concept trial
- PMID: 30466449
- PMCID: PMC6251087
- DOI: 10.1186/s12969-018-0292-3
Feasibility of a musculoskeletal ultrasound intervention to improve adherence in juvenile idiopathic arthritis: a proof-of concept trial
Abstract
Background: Non-adherence is a prevalent and modifiable issue in juvenile idiopathic arthritis (JIA) that currently lacks provider-based intervention. Education surrounding disease status is one way in which families remain engaged in their care. Musculoskeletal ultrasound is one such form of demonstrative, real-time education that may impact the way patients and caregivers self-manage their disease. The aims of this study are to 1) assess the feasibility, acceptability and perceived usefulness of musculoskeletal ultrasound as a non-adherence intervention tool and 2) to examine changes in methotrexate adherence in adolescents with JIA following the ultrasound.
Methods: Eight adolescents with polyarticular or extended oligoarticular JIA and their caregivers completed this 12 week study. A within subject design was used to compare baseline and post-intervention adherence, quality of life and disease activity indices. Adherence measures included electronic measurement of methotrexate in addition to self-reported adherence questionnaires. The ultrasound intervention included a one-time, rheumatologist provided, educational examination of three or more currently or historically active joints.
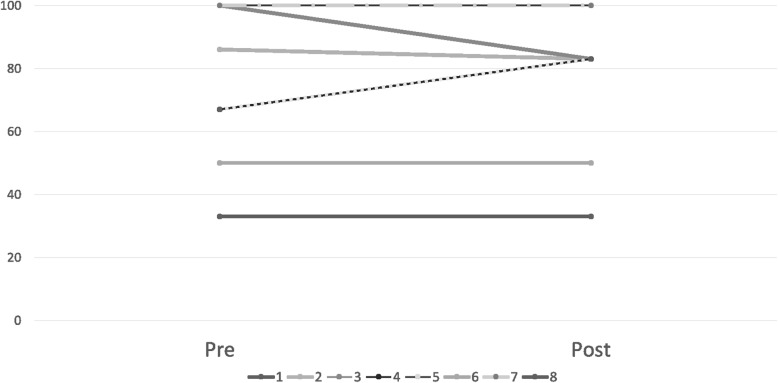
Results: The ultrasound intervention was found to be both feasible and acceptable. One hundred percent of eligible participants completed the ultrasound intervention. The ultrasound was well received by patients and caregivers, with most believing this to be a helpful tool. Baseline adherence was 75.3% among participants, with half of the participants being classified as non-adherent. Electronically measured and self-reported adherence measures did not show significant changes during the post-intervention period. Two participants improved, four participants maintained, and two participants decreased adherence. On ultrasound, 18/27 (66.7%) of the examined joints displayed abnormalities, with 63% being discrepant and additive to the rheumatologist's physical examination.
Conclusions: While our intervention did not show any changes in adherence, quality of life or disease activity indices in this proof-of-concept trial, the intervention does show promise in acceptability measures and merits future study in a more robust trial design. An additional study benefit was that the musculoskeletal ultrasound intervention was able to demonstrate subclinical disease, leading to clinically impactful therapeutic changes in several participants.
Keywords: Adherence; Juvenile idiopathic arthritis; Musculoskeletal ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
This study received Institutional Review Board Approval (#2016–9219) through Cincinnati Children’s Hospital Medical Center.
Consent for publication
All 11 adolescents who were enrolled completed a written assent and their respective caregivers completed a written consent to participate and have this work published.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


Similar articles
-
A wearable activity tracker intervention for promoting physical activity in adolescents with juvenile idiopathic arthritis: a pilot study.Pediatr Rheumatol Online J. 2018 Oct 22;16(1):66. doi: 10.1186/s12969-018-0282-5. Pediatr Rheumatol Online J. 2018. PMID: 30348203 Free PMC article.
-
Fluorescence optical imaging and musculoskeletal ultrasonography in juvenile idiopathic polyarticular disease before and during antirheumatic treatment - a multicenter non-interventional diagnostic evaluation.Arthritis Res Ther. 2017 Jun 30;19(1):147. doi: 10.1186/s13075-017-1355-4. Arthritis Res Ther. 2017. PMID: 28666454 Free PMC article.
-
The iPeer2Peer Program: a pilot randomized controlled trial in adolescents with Juvenile Idiopathic Arthritis.Pediatr Rheumatol Online J. 2016 Sep 2;14(1):48. doi: 10.1186/s12969-016-0108-2. Pediatr Rheumatol Online J. 2016. PMID: 27590668 Free PMC article. Clinical Trial.
-
Harnessing interactive technologies to improve health outcomes in juvenile idiopathic arthritis.Pediatr Rheumatol Online J. 2017 May 16;15(1):40. doi: 10.1186/s12969-017-0168-y. Pediatr Rheumatol Online J. 2017. PMID: 28511689 Free PMC article. Review.
-
Juvenile idiopathic arthritis - the role of imaging from a rheumatologist's perspective.Pediatr Radiol. 2018 Jun;48(6):785-791. doi: 10.1007/s00247-017-4014-7. Epub 2018 May 8. Pediatr Radiol. 2018. PMID: 29766250 Review.
Cited by
-
Musculoskeletal ultrasound in children: Current state and future directions.Eur J Rheumatol. 2020 Feb;7(Suppl1):S28-S37. doi: 10.5152/eurjrheum.2019.19170. Eur J Rheumatol. 2020. PMID: 35929859 Free PMC article.
-
Emergence of Musculoskeletal Ultrasound Use in Pediatric Rheumatology.Curr Rheumatol Rep. 2020 Apr 14;22(5):14. doi: 10.1007/s11926-020-0889-7. Curr Rheumatol Rep. 2020. PMID: 32291537 Review.
-
From image to insight: leveraging imaging to empower patients with inflammatory arthropathies.Front Med (Lausanne). 2025 Aug 8;12:1630114. doi: 10.3389/fmed.2025.1630114. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40861224 Free PMC article. Review.
-
Feasibility and acceptability of an innovative adherence intervention for young adults with childhood-onset systemic Lupus Erythematosus.Pediatr Rheumatol Online J. 2020 Apr 26;18(1):36. doi: 10.1186/s12969-020-00430-z. Pediatr Rheumatol Online J. 2020. PMID: 32340616 Free PMC article. Clinical Trial.
-
Musculoskeletal Ultrasound in Childhood Arthritis Limited Examination: A Comprehensive, Reliable, Time-Efficient Assessment of Synovitis.Arthritis Care Res (Hoboken). 2023 Feb;75(2):401-409. doi: 10.1002/acr.24759. Epub 2022 Sep 13. Arthritis Care Res (Hoboken). 2023. PMID: 34328679 Free PMC article.
References
-
- Wallace CA, Giannini EH, Spalding SJ, Hashkes PJ, O’Neil KM, Zeft AS, et al. Clinically inactive disease in a cohort of children with new-onset polyarticular juvenile idiopathic arthritis treated with early aggressive therapy: time to achievement, total duration, and predictors. J Rheumatol. 2014;41(6):1163–1170. doi: 10.3899/jrheum.131503. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
