

Minimally invasive drainage in critically ill patients with severe necrotizing pancreatitis is associated with better outcomes: an observational study
- PMID: 30466472
- PMCID: PMC6249885
- DOI: 10.1186/s13054-018-2256-x
Minimally invasive drainage in critically ill patients with severe necrotizing pancreatitis is associated with better outcomes: an observational study
Abstract
Background: Infected pancreatic necrosis, which occurs in about 40% of patients admitted for acute necrotizing pancreatitis, requires combined antibiotic therapy and local drainage. Since 2010, drainage by open surgical necrosectomy has been increasingly replaced by less invasive methods such as percutaneous radiological drainage, endoscopic necrosectomy, and laparoscopic surgery, which proved effective in small randomized controlled trials in highly selected patients. Few studies have evaluated minimally invasive drainage methods used under the conditions of everyday hospital practice. The aim of this study was to determine whether, compared with conventional open surgery, minimally invasive drainage was associated with improved outcomes of critically ill patients with infection complicating acute necrotizing pancreatitis.
Methods: A single-center observational study was conducted in patients admitted to the intensive care unit for severe acute necrotizing pancreatitis to compare the characteristics, drainage techniques, and outcomes of the 62 patients managed between September 2006 and December 2010, chiefly with conventional open surgery, and of the 81 patients managed between January 2011 and August 2015 after the introduction of a minimally invasive drainage protocol.
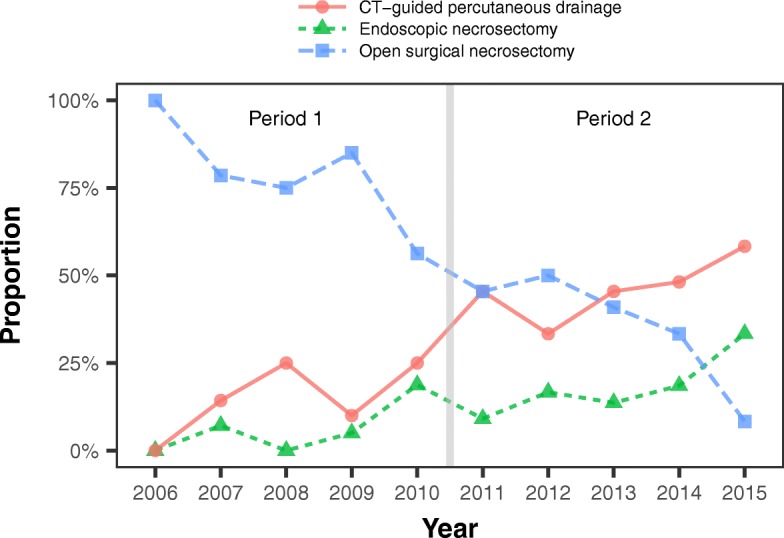
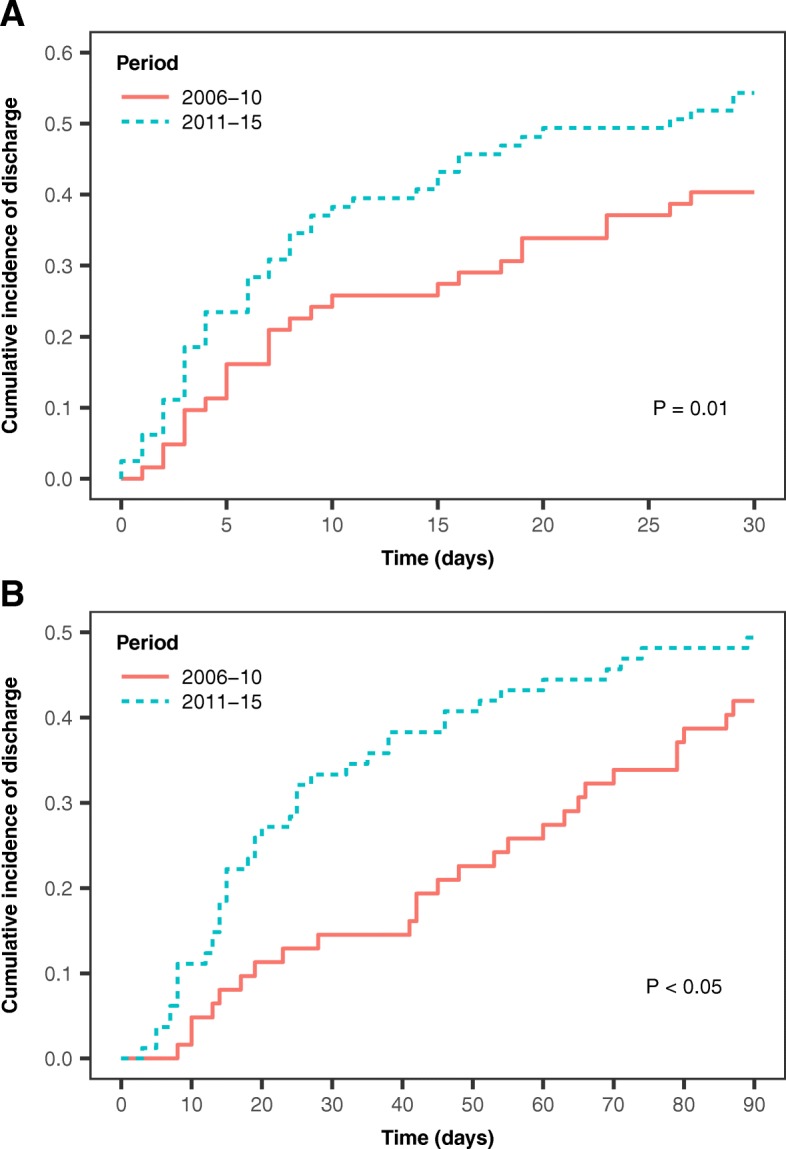
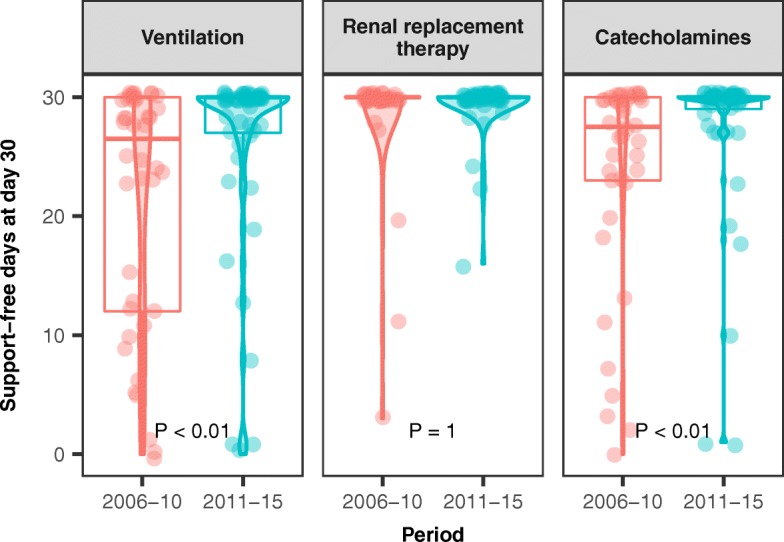
Results: Surgical necrosectomy was more common in the early period (74% versus 41%; P <0.001), and use of minimally invasive drainage increased between the early and late periods (19% and 52%, respectively; P <0.001). The numbers of ventilator-free days and catecholamine-free days by day 30 were higher during the later period. The proportions of patients discharged from intensive care within the first 30 days and from the hospital within the first 90 days were higher during the second period. Hospital mortality was not significantly different between the early and late periods (19% and 22%, respectively).
Conclusion: In our study, the implementation of a minimally invasive drainage protocol in patients with infected pancreatic necrosis was associated with shorter times spent with organ dysfunction, in the intensive care unit, and in the hospital. Mortality was not significantly different. These results should be interpreted bearing in mind the limitations inherent in the before-after study design.
Keywords: Infected pancreatic necrosis; Severe acute pancreatitis; Step-up approach; Surgical pancreatic necrosectomy.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the French Data Protection Authority (
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
