

Diagnostic performance of abdominal point of care ultrasound performed by an emergency physician in acute right iliac fossa pain
- PMID: 30467798
- PMCID: PMC6250608
- DOI: 10.1186/s13089-018-0112-5
Diagnostic performance of abdominal point of care ultrasound performed by an emergency physician in acute right iliac fossa pain
Abstract
Background: Right iliac fossa abdominal pain is a common reason for emergency ward admissions, its etiology is difficult to diagnose. It can be facilitated by an imaging examination, such as a Computerized Tomography scan which exposes the patient to ionizing radiation and implies delays. A bedside ultrasound performed by emergency physicians could avoid these issues. The aim of our study was to assess the performance of ultrasound carried out at the patient's bedside by an emergency physician compared with a clinical-laboratory examination for the diagnosis of a surgical pathology in right iliac fossa pain.
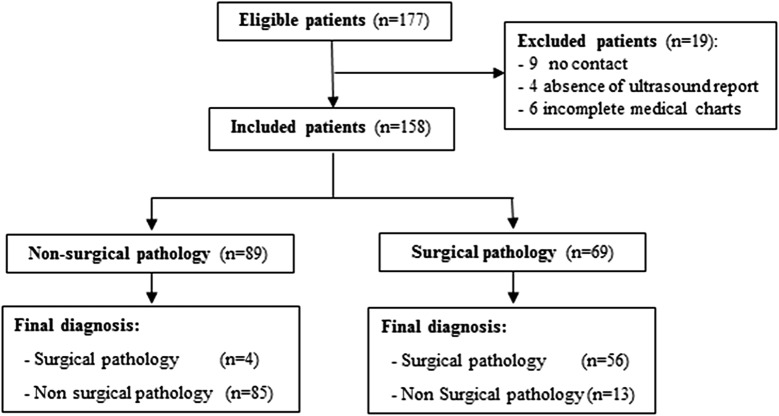
Methods: This is a single-center prospective cohort study conducted in an Emergency Department receiving 19,000 patients per year. All patients presenting pain in the right iliac fossa were included by four (out of ten) emergency physicians certified in an ultrasound examination. A full grid pattern scan ultrasound of the abdominal cavity with analysis of the right iliac fossa was performed. The primary outcome was to compare the diagnosis performance of bedside ultrasound and clinical-laboratory examination to detect a surgical pathology. Two emergency physicians who did not participate in the study made the final diagnosis (i.e., surgical or non-surgical pathology) by reviewing the entire medical chart of each patient.
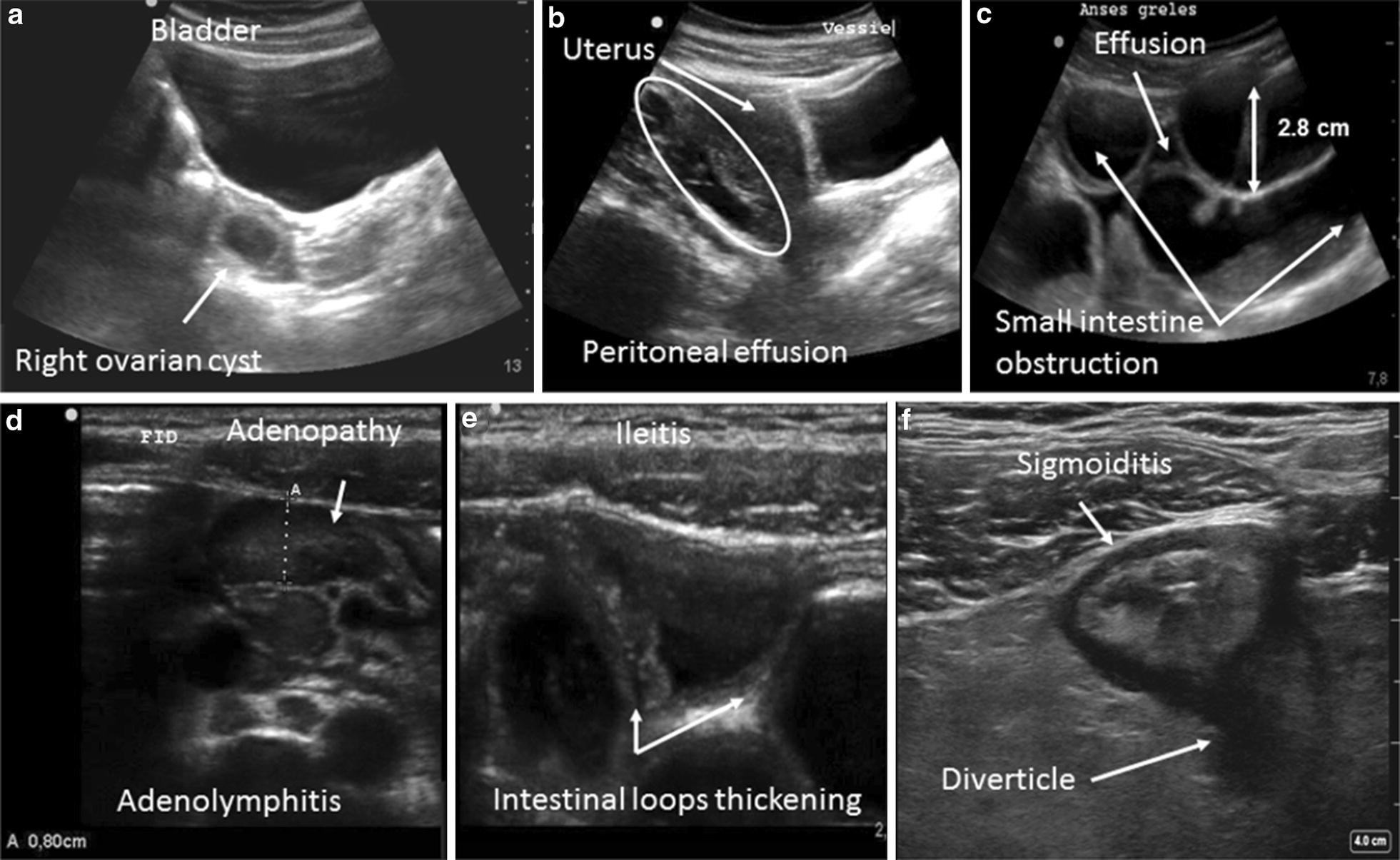
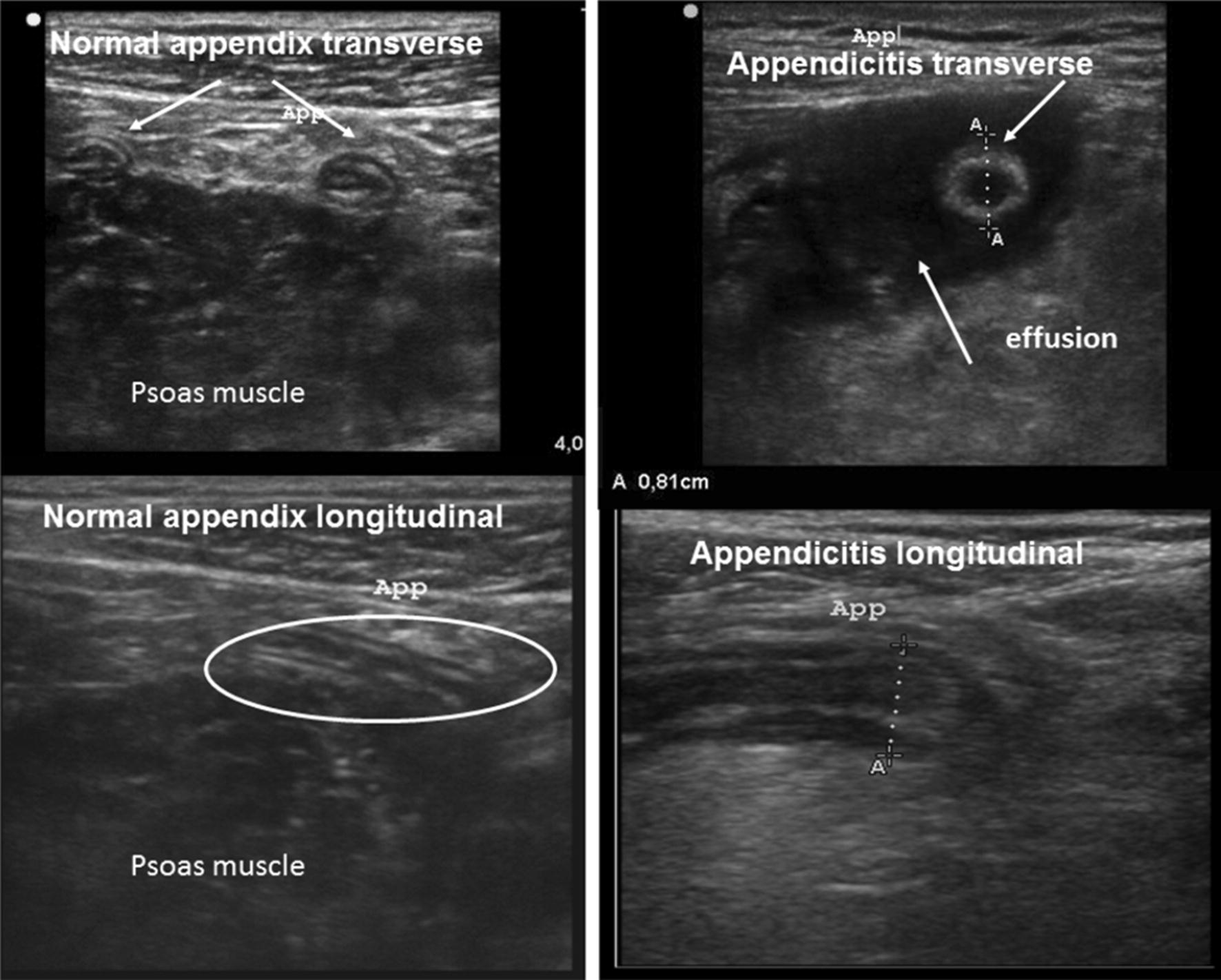
Results: From January 2011 to July 2013, 158 patients with a median age of 17 [13-32] years were analyzed. The diagnosed cases were: appendicitis (53), non-specific abdominal pain (48), lymphadenitis (22), ileitis (11), complicated ovarian cysts (7), neoplasias (5), inflammatory or infectious colitis (5), inguinal herniations (3), bowel obstructions (2), and salpingitis (2). The accuracy of ultrasound diagnoses was 0.89 (95% CI 0.84-0.94) versus 0.70 (95% CI 0.57-0.82) for diagnoses based on clinical-laboratory examination only (p < 0.001).
Conclusion: Bedsides, ultrasound allows an accurate diagnosis of a surgical pathology in 89% of cases, which is more efficient than the clinical-laboratory examination.
Keywords: Abdominal pain; Appendicitis; Bedside ultrasound; Diagnostic methods.
Figures
References
-
- Stone R. Acute abdominal pain. Lippincotts Prim Care Pract. 1998;2(4):341–357. - PubMed
LinkOut - more resources
Full Text Sources
