

doi: 10.1016/j.jaci.2018.10.057.
Epub 2018 Nov 20.
Interlaboratory variability in multiplexed pneumococcal antibody testing
Affiliations
- PMID: 30468776
- PMCID: PMC6684100
- DOI: 10.1016/j.jaci.2018.10.057
Item in Clipboard
Interlaboratory variability in multiplexed pneumococcal antibody testing
J Allergy Clin Immunol.
2019 Mar.
Erratum in
-
Corrigenda.J Allergy Clin Immunol. 2019 Aug;144(2):626. doi: 10.1016/j.jaci.2019.06.005. J Allergy Clin Immunol. 2019. PMID: 31395152 No abstract available.
Abstract
This pragmatic, updated assessment of variability among pneumococcal antibody assays suggests that variability may now be greater than previously reported, and potentially influential in clinical decision making.
Conflict of interest statement
Figures
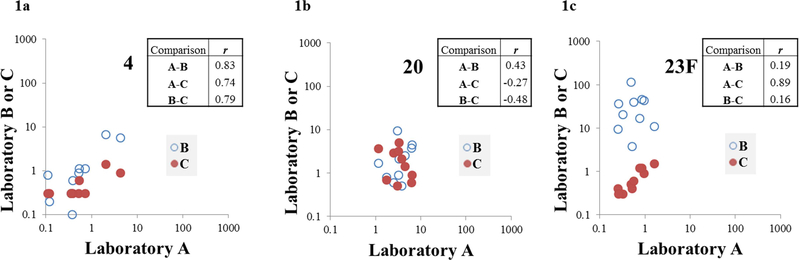
X axis values represent pneumococcal IgG antibody levels (μg/ml)
for laboratory A, with Y axis values representing antibody levels from
laboratories B (open circle) or C (solid circle). Boxes show correlation
coefficients (r) for each inter-laboratory comparison. There
was strong correlation (r ≥0.70) across all three
comparisons for only one serotype (serotype 4, Figure 1a). There was weak
correlation (r ≤0.50) for all three comparisons for four
serotypes (including serotype 20, Figure 1b). There was strong correlation
between A and C, with weaker correlation for other comparisons for eight
serotypes (including serotype 23F, Figure 1c).
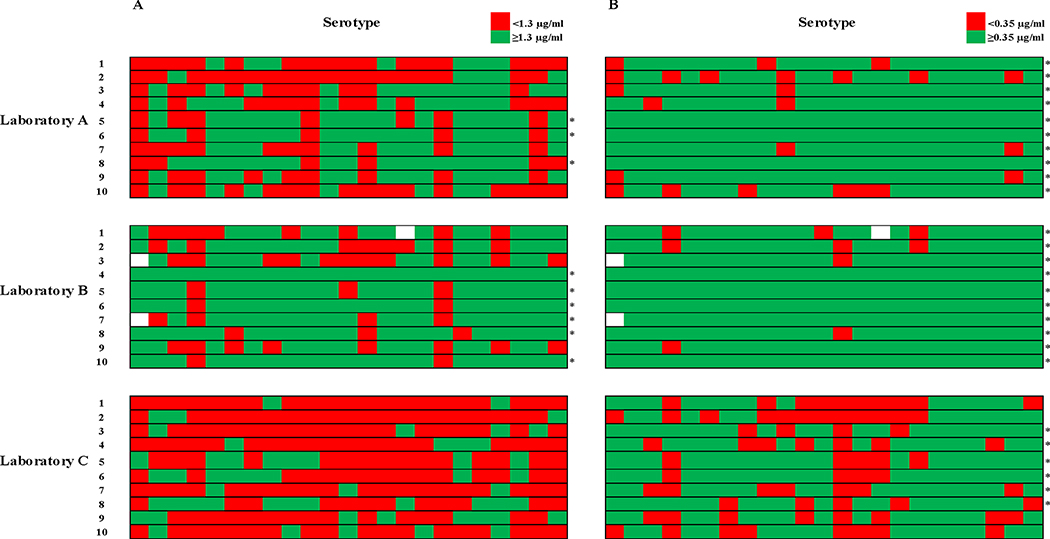
Individual measurements were categorized as nonprotective or protective
on the basis of the specified thresholds, and are represented by red and green
shaded boxes, respectively. Numbered rows represent serum samples, with columns
representing serotypes. An asterisk to the right of a sample’s row
indicates overall “protected” status for that sample (at least 70%
of serotypes at or above the protective threshold). Empty boxes indicate three
missing measurements from laboratory B (serotype 1 from two samples, and 15B
from another), which was unable to analyze these serotypes due to a non-linear
dilution response for those samples. 2a. Classification of pneumococcal IgG levels based on AAAAI
criteria. A threshold of 1.3 μg/ml was used to categorize
individual measurements as nonprotective (<1.3 μg/ml, red shaded
boxes) or protective (≥1.3 μg/ml, green shaded boxes). 2b. Classification of pneumococcal IgG levels based on the WHO
recommendations for pneumococcal vaccine evaluation. A threshold of
0.35 μg/ml was used to categorize individual measurements as
nonprotective (<0.35 μg/ml, red shaded boxes) or protective
(≥0.35 μg/ml, green shaded boxes).
References
-
- Orange JS, Ballow M, Stiehm ER, Ballas ZK, Chinen J, De La Morena M, et al. Use and interpretation of diagnostic vaccination in primary immunodeficiency: a working group report of the Basic and Clinical Immunology Interest Section of the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2012;130(3 Suppl):S1–24. - PubMed
-
- Sorensen RU, Leiva LE, Javier FC 3rd, Sacerdote DM, Bradford N, Butler B, et al. Influence of age on the response to Streptococcus pneumoniae vaccine in patients with recurrent infections and normal immunoglobulin concentrations. J Allergy Clin Immunol. 1998;102(2):215–21. - PubMed
-
- Beck SC. Making sense of serotype-specific pneumococcal antibody measurements. Ann Clin Biochem. 2013;50(Pt 6): 517–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
