

Implementation of a co-designed physical activity program for older adults: positive impact when delivered at scale
- PMID: 30470209
- PMCID: PMC6251145
- DOI: 10.1186/s12889-018-6210-2
Implementation of a co-designed physical activity program for older adults: positive impact when delivered at scale
Abstract
Background: Despite known health benefits of physical activity (PA), older adults remain among the least physically active age group globally with 30-60% not meeting guidelines. In Canada, 87% do not meet recommended guidelines. To influence population health, interventions that are effective in small trials must be disseminated at scale. Despite evidence for efficacy, few PA interventions are scaled up to reach the wider community. In 2015, British Columbia (BC) Ministry of Health released a PA strategy where older adults were identified as a priority. In partnership with the Ministry, the Active Aging Research Team co-created a health promotion program called Choose to Move (CTM). CTM will be implemented in three phases at increasingly greater scale across BC. The objective of this study is to evaluate the effectiveness of CTM during Phase I (pilot) and Phase II (initial scale up) on PA, mobility, and social connectedness among older adults in BC, Canada.
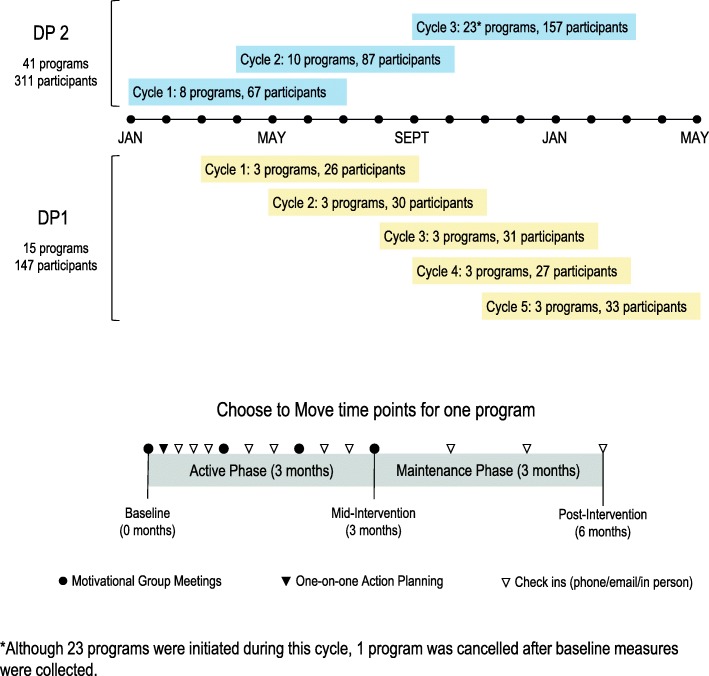
Methods: We used a type 2 hybrid effectiveness-implementation study design, and herein focus on effectiveness. The implementation evaluation will be published as a companion paper elsewhere. Two community delivery partner organizations delivered 56 CTM programs in 26 large and small urban locations across BC. Outcome measurement occurred at 0 (baseline), 3 (mid-intervention) and 6 (post-intervention) months. We collected survey data from all participants (n = 458; province-wide) and also conducted a subset evaluation (n = 209).
Results: PA increased significantly during the active intervention phase (baseline-3 months) in younger (60-74 yrs.; + 1.6 days/week; p < 0.001) and older (≥75 yrs.; + 1.0 days/week; p < 0.001) participants. The increase was sustained at 6 months in younger participants only, who remained significantly more active than at baseline (+ 1.4 days/week; p < 0.001). Social exclusion indicators declined significantly in the younger group. Mobility and strength improved significantly at 3 months in the younger group, and in both groups at 6 months.
Conclusions: CTM adopted central tenets of implementation science that consider the complicated systems where interventions are delivered to improve public health. In this iteration of CTM we demonstrate that a partner-based health promotion intervention can be effectively implemented across settings to enhance PA, mobility and social connectedness in older adults.
Keywords: Impact evaluation; Implementation science; Mobility; Older adults; Physical activity; Scale up; Seniors; Social connectedness.
Conflict of interest statement
Ethics approval and consent to participate
The UBC and SFU Clinical Research Ethics Boards (H15–02522 (UBC) and 22,015 s0614 (SFU)) approved all study procedures. All participants provided informed written consent prior to providing data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Statistics Canada: Age and sex, and type of dwelling data: key results from the 2016 census. The Daily 2017. https://www150.statcan.gc.ca/n1/daily-quotidien/170503/dq170503a-eng.htm. Accessed 20 Sept 2017.
-
- Statistics Canada . Canadian demographics at a glance. 2016.
-
- Heikkinen R. WHO ageing and health Programme: growing older - staying well: ageing and physical activity in everyday life. In: Institutional Repository for Information Sharing. Geneva: World Health Organization; 1998.
-
- Guralnik JM, Ferrucci L, Pieper CF, Leveille SG, Markides KS, Ostir GV, Studenski S, Berkman LF, Wallace RB. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci. 2000;55(4):M221–M231. doi: 10.1093/gerona/55.4.M221. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
