

A systematic review of the cost and cost-effectiveness studies of immune checkpoint inhibitors
- PMID: 30470252
- PMCID: PMC6251215
- DOI: 10.1186/s40425-018-0442-7
A systematic review of the cost and cost-effectiveness studies of immune checkpoint inhibitors
Abstract
Background: Escalating healthcare costs are necessitating the practice of value-based oncology. It is crucial to critically evaluate the economic impact of influential but expensive therapies such as immune checkpoint inhibitors (ICIs). To date, no systematic assessment of the cost-effectiveness (CE) of ICIs has been performed.
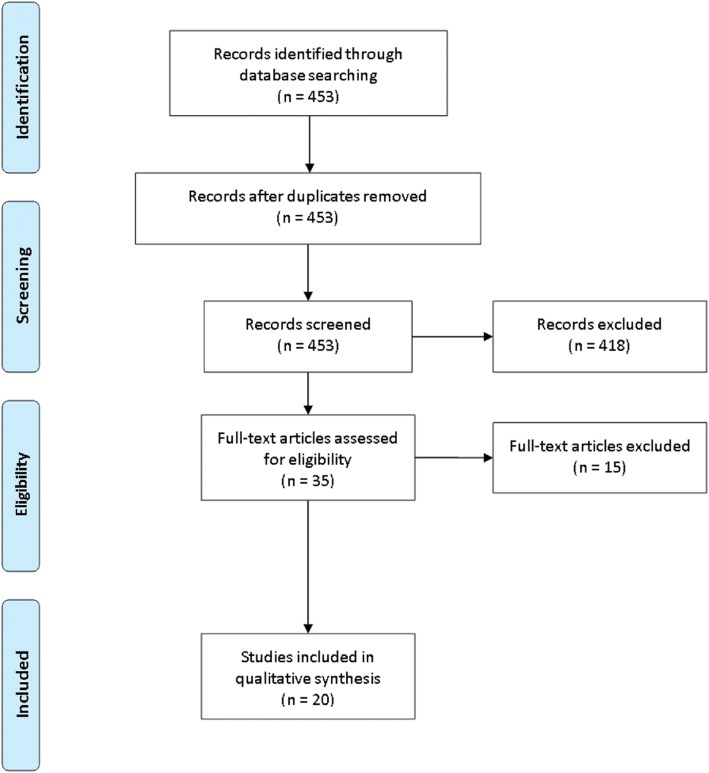
Methods: PRISMA-guided systematic searches of the PubMed database were conducted. Studies of head/neck (n = 3), lung (n = 5), genitourinary (n = 4), and melanoma (n = 8) malignancies treated with ICIs were evaluated. The reference willingness-to-pay (WTP) threshold was $100,000/QALY.
Results: Nivolumab was not cost-effective over chemotherapy for recurrent/metastatic head/neck cancers (HNCs). For non-small cell lung cancer (NSCLC), nivolumab was not cost-effective for a general cohort, but increased PD-L1 cutoffs resulted in CE. Pembrolizumab was cost-effective for both previously treated and newly-diagnosed metastatic NSCLC. For genitourinary cancers (GUCs, renal cell and bladder cancers), nivolumab and pembrolizumab were not cost-effective options. Regarding metastatic/unresected melanoma, ipilimumab monotherapy is less cost-effective than nivolumab, nivolumab/ipilimumab, and pembrolizumab. The addition of ipilimumab to nivolumab monotherapy was not adequately cost-effective. Pembrolizumab or nivolumab monotherapy offered comparable CE profiles.
Conclusions: With limited data and from the reference WTP, nivolumab was not cost-effective for HNCs. Pembrolizumab was cost-effective for NSCLC; although not the case for nivolumab, applying PD-L1 cutoffs resulted in adequate CE. Most data for nivolumab and pembrolizumab in GUCs did not point towards adequate CE. Contrary to ipilimumab, either nivolumab or pembrolizumab is cost-effective for melanoma. Despite these conclusions, it cannot be overstated that careful patient selection is critical for CE. Future publication of CE investigations and clinical trials (along with longer follow-up of existing data) could substantially alter conclusions from this analysis.
Keywords: Cost-effectiveness; Health policy; Immune checkpoint inhibitor; Immunotherapy; Public health; Public policy; Value.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable secondary to no use of human data.
Consent for publication
Not applicable secondary to no use of human data.
Competing interests
JWW declares the following conflicts of interest: He is a co-founder of Healios, MolecularMatch, and OncoResponse. He is a scientific board advisor for Reflexion Medical, Checkmate Pharmaceuticals, and Mavu; and he receives clinical research support from BMS and Merck and laboratory research support from Varian, Incyte, Merck, Calithera, Checkmate Pharmaceuticals, and OncoResponse.
All other authors have no conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- American Cancer Society. Immune Checkpoint Inhibitors to Treat Cancer. https://www.cancer.org/treatment/treatments-and-side-effects/treatment-t.... Accessed 4 Apr 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials