

Review
doi: 10.1067/j.cpsurg.2018.07.001.
Epub 2018 Aug 8.
Robotic gastrointestinal surgery
Affiliations
- PMID: 30470267
- PMCID: PMC6377083
- DOI: 10.1067/j.cpsurg.2018.07.001
Item in Clipboard
Review
Robotic gastrointestinal surgery
Curr Probl Surg.
2018 Jun.
No abstract available
Figures
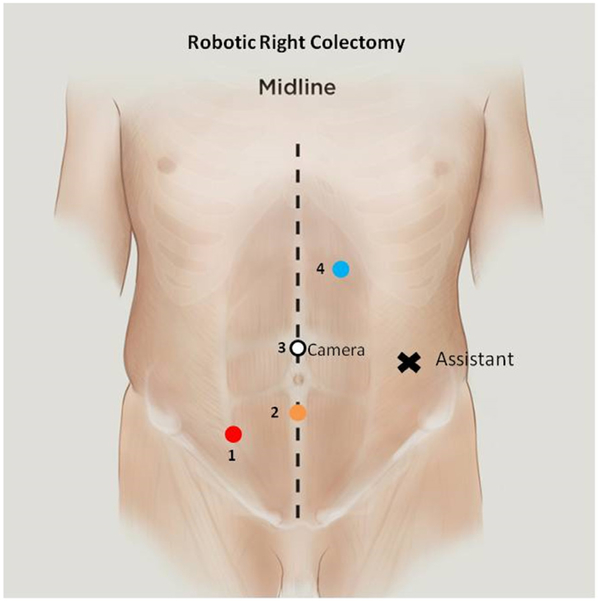
Robotic right colectomy port positions.
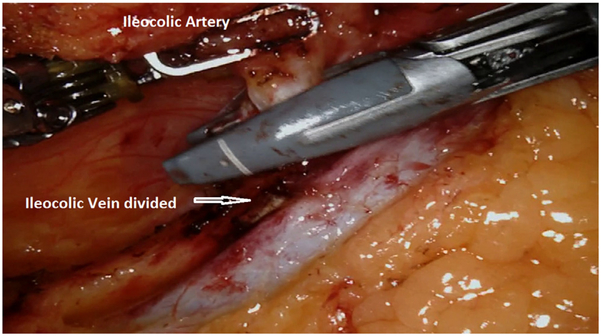
Ileocolic artery division. The ileocolic vein has been previously divided using the vessel sealer.
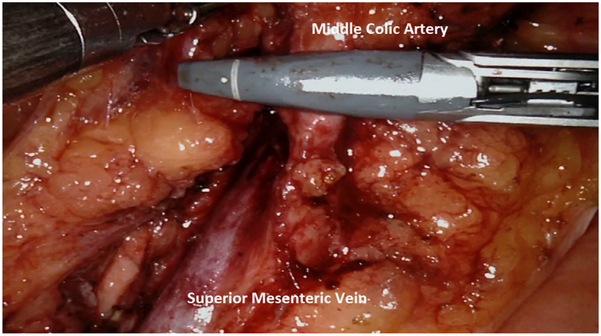
Division of the middle colic artery using a vessel sealer.
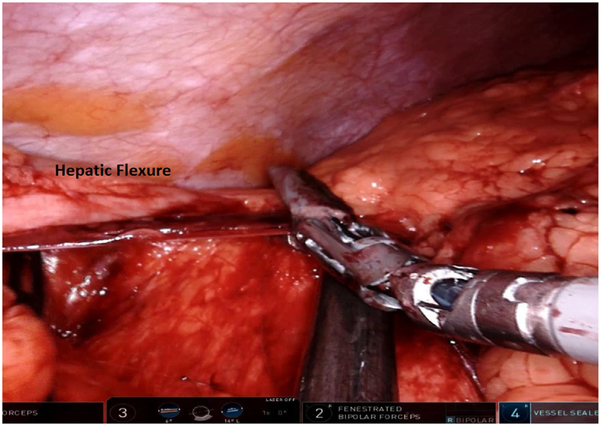
Dissection of the hepatic flexure.
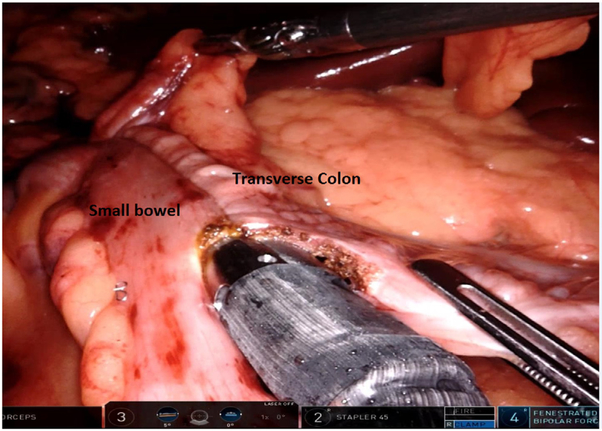
Intracorporeal isoperistaltic anastomosis between the terminal ileum and transverse colon.
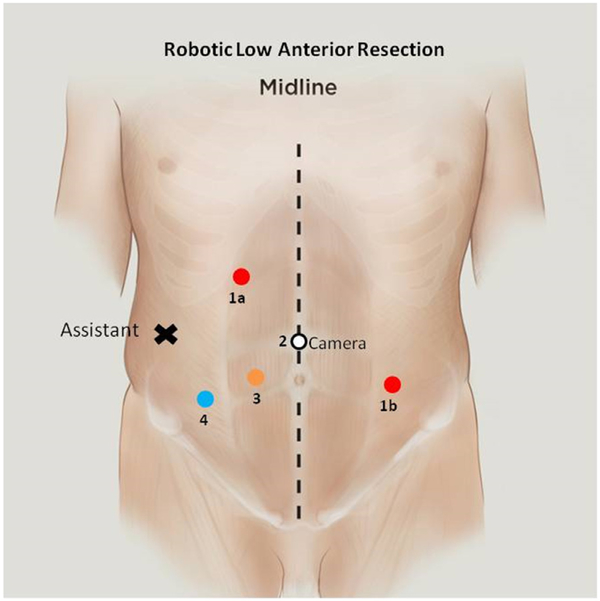
Port placement for robotic low anterior resection. For pedicle ligation and splenic flexure, mobilization ports 1a, 2, and 3 are used. For pelvic dissection, ports 1b, 2, and 3 are used.
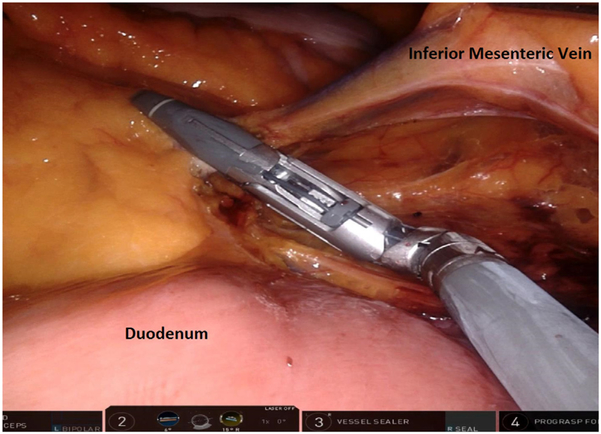
Inferior mesenteric vein dissected adjacent to the ligament of Treitz and inferior border of the pancreas before division.
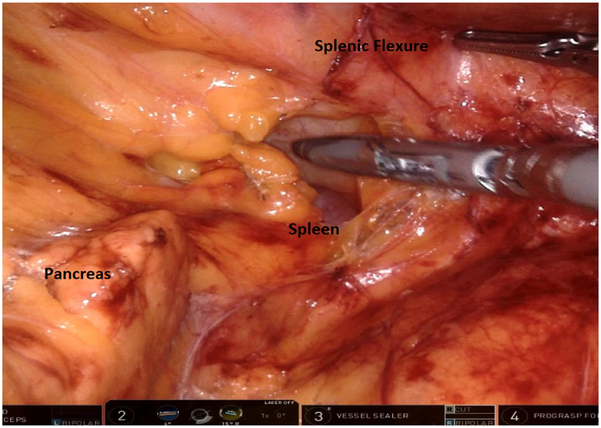
Medial-to-lateral dissection revealing the pancreas, prior to visualization of the spleen. The splenic flexure of the colon is gently retracted using the grasper.
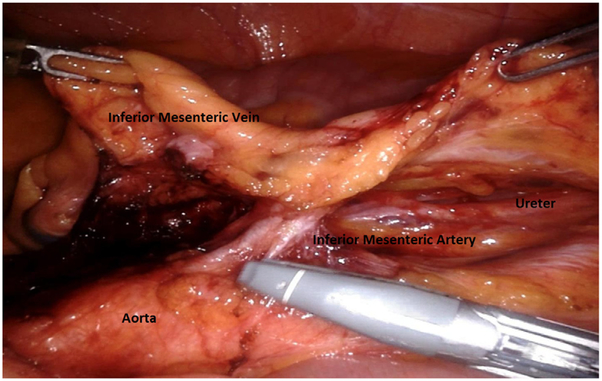
Inferior mesenteric artery (note characteristic T-shaped structure) after dividing the inferior mesenteric vein. The ureter and gonadal vessels are visible prior to artery division.

Posterior mesorectal excision plane. The hypogastric nerves are swept lateral during dissection.
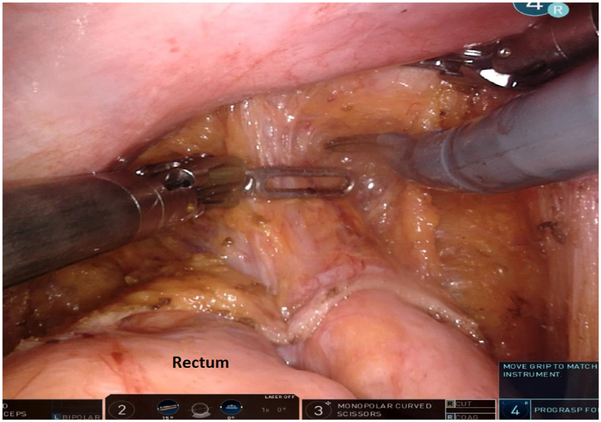
After the peritoneal plane is incised, dissection should continue along the rectovaginal septum in women or rectovesical fascia in men.
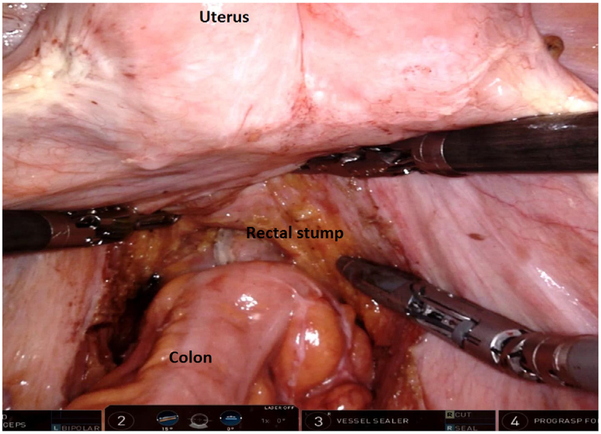
End-to-end intracorporeal stapled anastomosis between the descending colon and the rectal stump. The pelvic space is completely exposed, and the uterus can be retracted using a stitch.
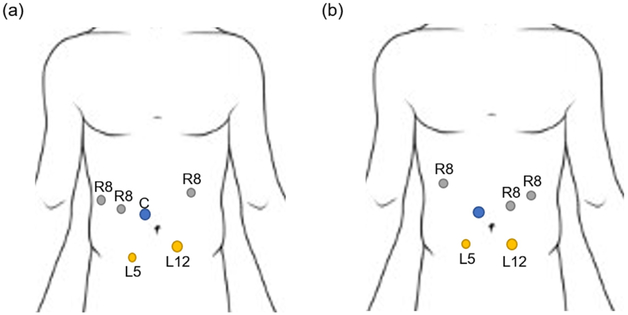
Port placements for (a) robotic pancreaticoduodenectomy, and (b) robotic distal pancreatectomy. C: Camera port, R8: 8 mm robotic trocar, L5: 5 mm laparoscopic trocar, L12: 12 mm laparoscopic trocar.
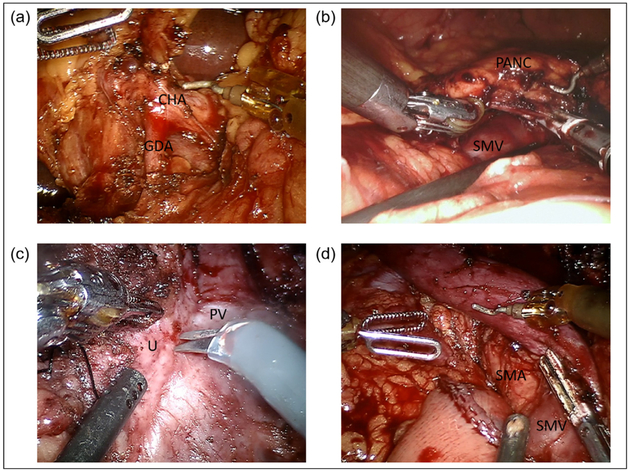
Robotic pancreaticoduodenectomy dissection and resection. (a) Porta hepatis dissection and identification of the gastroduodenal artery during robotic pancreaticoduodenectomy. (b) Creation of retropancreatic tunnel anterior to the superior mesenteric vein along the inferior border of the pancreatic neck. (c) Uncinate process dissection. (d) Completed dissection demonstrating exposed superior mesenteric vein, superior mesenteric artery and proximal jejunum. CHA, common hepatic artery; GDA, gastroduodenal artery; PANC, pancreas; PV, portal vein; SMA, superior mesenteric artery; SMV, superior mesenteric vein; U, uncinate.
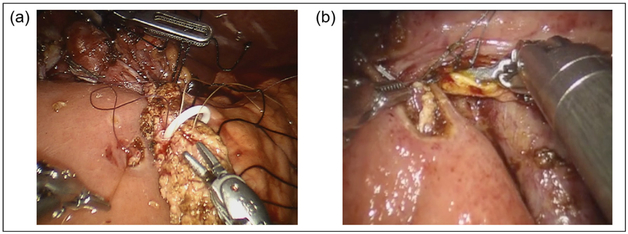
Robotic pancreaticoduodenectomy reconstruction. (a) Modified Blumgart pancreaticojejunostomy with pancre atic stent in place. (b) Continuous running hepaticojejunostomy.
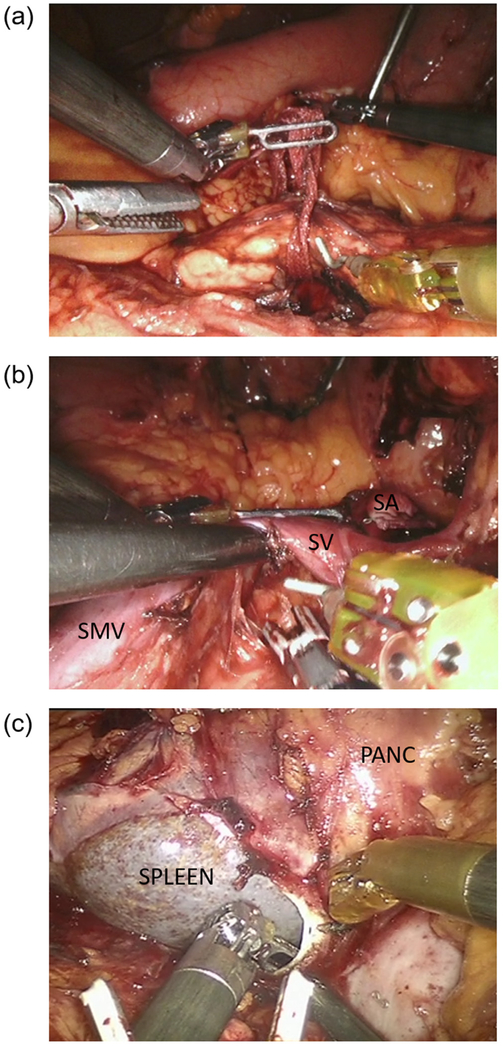
Robotic distal pancreatectomy dissection. (a) Creation of retropancreatic tunnel and passage of moist umbilical tape for upwards traction. (b) Division of the splenic artery at its takeoff and identification of the splenic vein for concurrent splenectomy. (c) Medial to lateral dissection of the pancreas and posterior pancreatic fascia. PANC, pancreas; SA, splenic artery; SMV, superior mesenteric vein; SV, splenic vein.
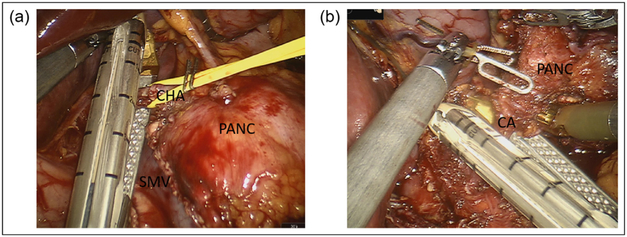
Robotic distal pancreatectomy with celiac axis resection. (a) Dissection and division of the common hepatic artery, ensuring protection of the gastroduodenal artery. (b) Transection of the celiac axis after circumferential dissection and lymphadenectomy. CA, celiac axis; CHA, common hepatic artery; PANC, pancreas; SMV, superior mesenteric vein.

Robotic total pancreatectomy with islet autotransplantation. (a) Dissection of the whole pancreas without division at the neck. Gastroduodenal artery, inferior mesenteric vein, and splenic vessels preserved until dissection is complete. (b) Splenic vein cannulation for infusion of autoislets. GDA, gastroduodenal artery; PANC, pancreas.
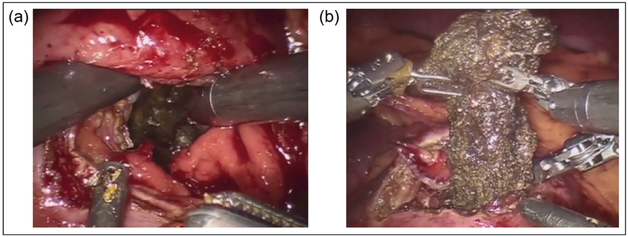
Robotic cyst gastrostomy. (a) Cyst gastrostomy performed with anterior and posterior gastrostomy into walled off necrosis of the pancreas. (b) Debridement of pancreatic necrosis.
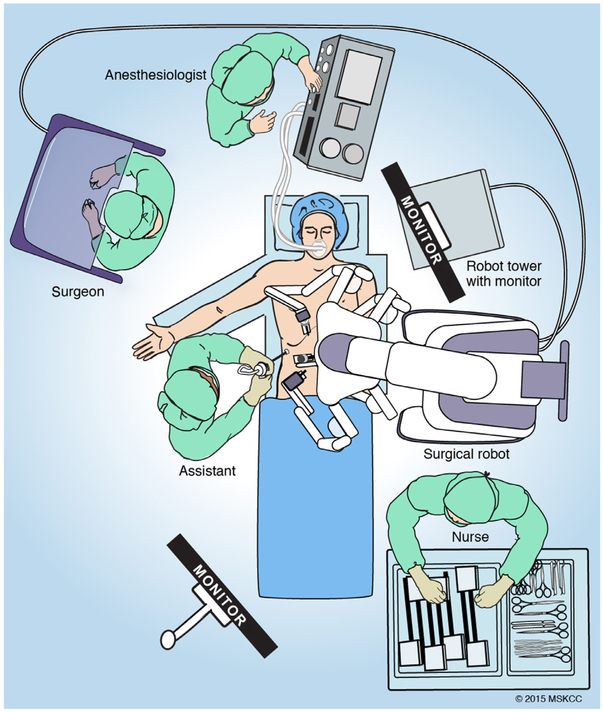
Position for a patient undergoing robotic total gastrectomy. Of note, the operation is generally performed in steep reverse Trendelenburg position and the patient must be positioned prior to docking the robot.
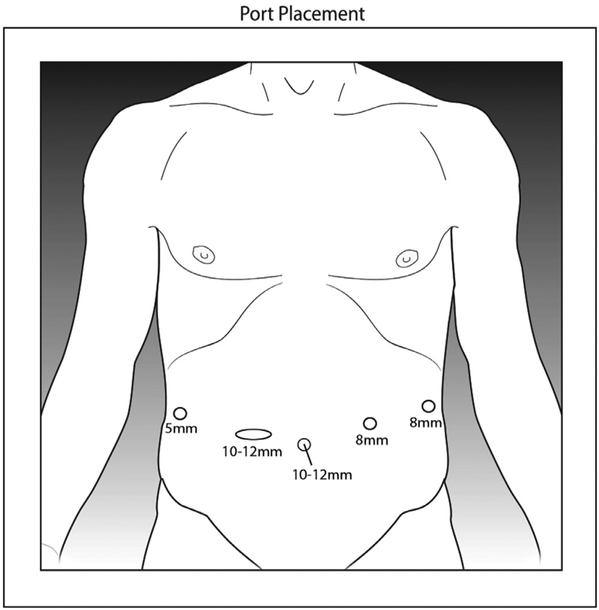
Recommended port placement for robotic gastrectomy.
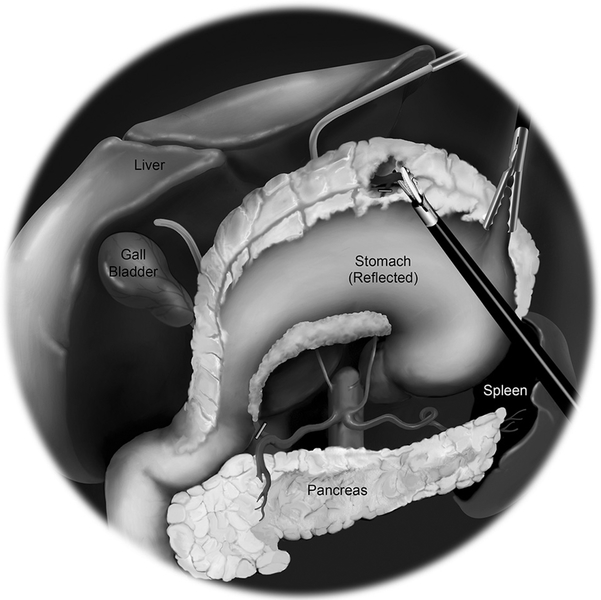
Entering the lesser sac and visualizing the posterior wall of the stomach allows the omentectomy to proceed safely to the splenic flexure.
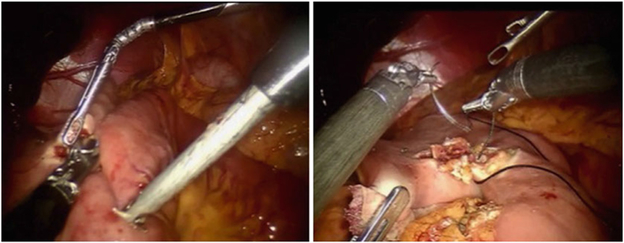
Confluence of right gastroepiploic and right colic veins at anterior border of pancreas.
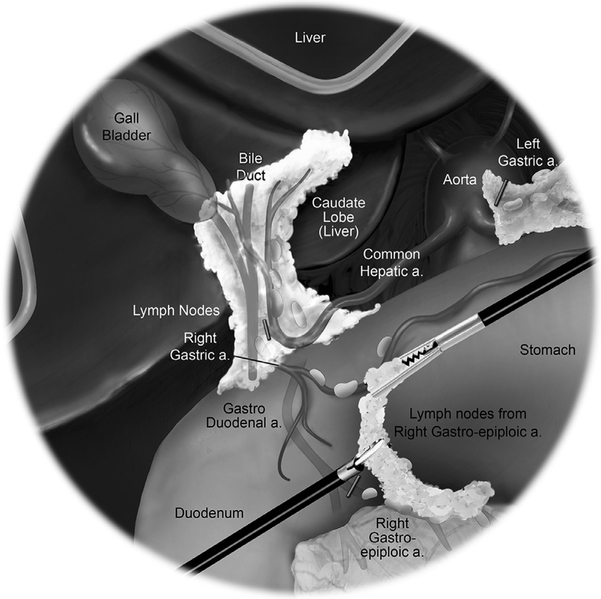
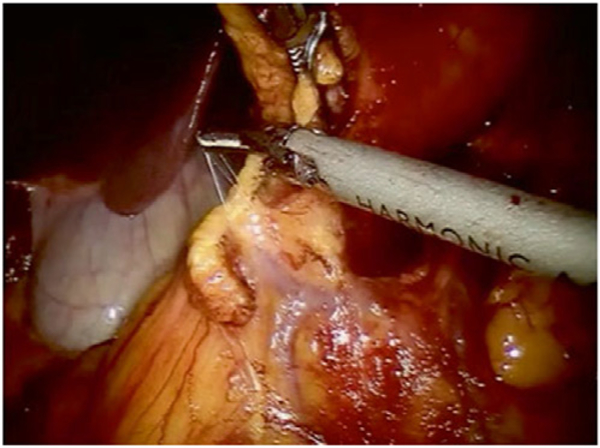
View of the proximal duodenum during dissection of the lymph nodes from the right gastroepiploic artery.
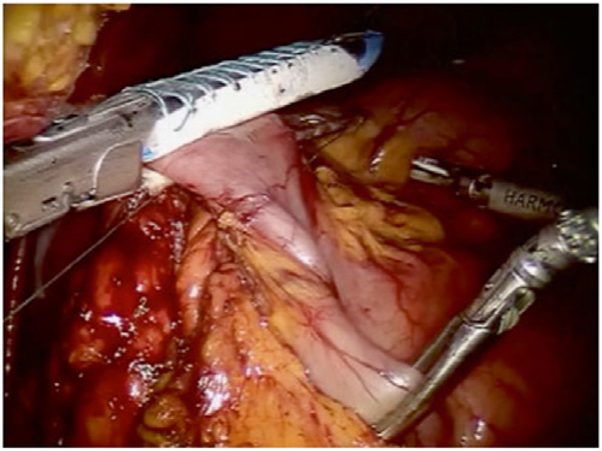
Division of proximal duodenum just distal to the pylorus.
(a) Creation of stapled side-to-side gastrojejunostomy. (b) Closure of gastroenterotomy.
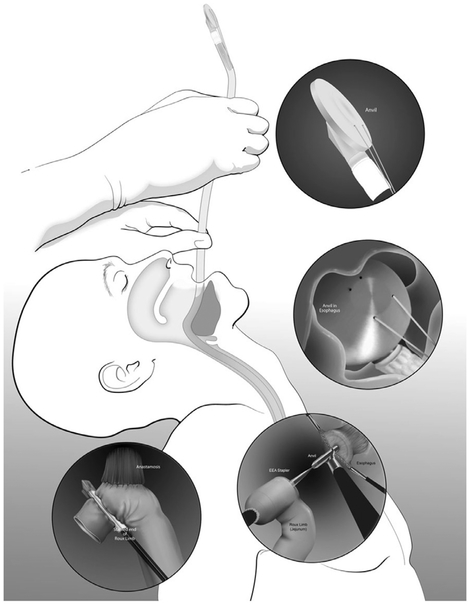
Use of a transoral anvil for construction of the esophagojejunostomy during total gastrectomy.
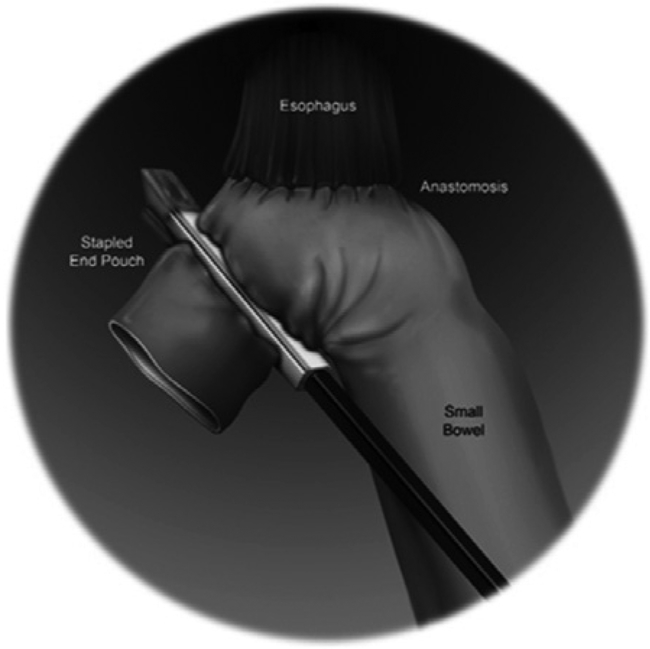
Schematic diagram of stapled esophagojejunostomy following total gastrectomy.
References
-
- Peterson CY, Weiser MR. Robotic colorectal surgery. J Gastrointest Surg. 2014;18:398–403. - PubMed
-
- Smith JJ, Weiser MR. Outcomes in non-metastatic colorectal cancer. J Surg Oncol. 2014;110:518–526. - PubMed
-
- Intuitive Surgical Inc. Intuitive Surgical’s EndoWrist Instruments http://www.intuitivesurgicalcom/products/instruments, Date Accessed October 1, 2017.
-
- Pappou EP, Weiser MR. Robotic colonic resection. J Surg Oncol. 2015;112:315–320. - PubMed
-
- Baek SJ, Kim CH, Cho MS, et al. Robotic surgery for rectal cancer can overcome difficulties associated with pelvic anatomy. Surg Endosc. 2015;29:1419–1424. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
