

Responsiveness and minimally important difference of SF-6D and EQ-5D utility scores for the treatment of pelvic organ prolapse
- PMID: 30471259
- PMCID: PMC6401219
- DOI: 10.1016/j.ajog.2018.11.1094
Responsiveness and minimally important difference of SF-6D and EQ-5D utility scores for the treatment of pelvic organ prolapse
Abstract
Background: Utility preference scores are standardized, generic, health-related quality of life (HRQOL) measures that quantify disease severity and burden and summarize morbidity on a scale from 0 (death) to 1 (optimal health). Utility scores are widely used to measure HRQOL and in cost-effectiveness research.
Objective: To determine the responsiveness, validity properties, and minimal important difference (MID) of utility scores, as measured by the Short Form 6D (SF-6D) and EuroQol (EQ-5D), in women undergoing surgery for pelvic organ prolapse (POP).
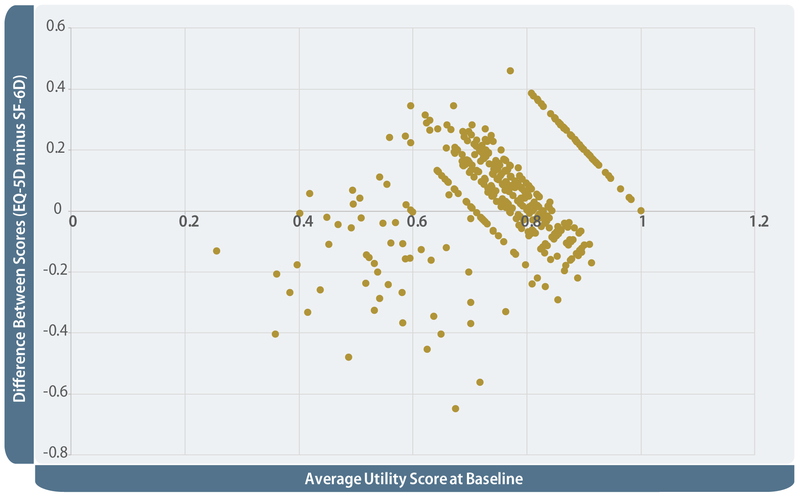
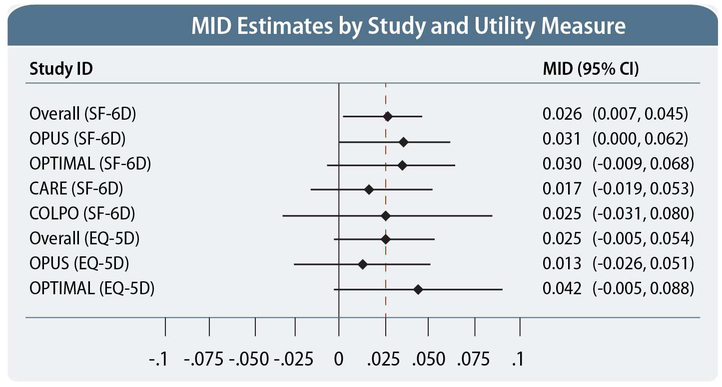
Materials and methods: This study combined data from 4 large, U.S., multicenter surgical trials enrolling 1321 women with pelvic organ prolapse. We collected condition-specific quality of life data using the Pelvic Floor Distress Inventory (PFDI) and Pelvic Floor Impact Questionnaire (PFIQ). A subset of women completed the SF6D; women in 2 trials also completed the EQ5D. Mean utility scores were compared from baseline to 12 months after surgery. Responsiveness was assessed using effect size (ES) and standardized response mean (SRM). Validity properties were assessed by (1) comparing changes in utility scores at 12 months between surgical successes and failures as defined in each study, and (2) correlating changes in utility scores with changes in the PFDI and PFIQ. MID was estimated using both anchor-based (SF-36 general health global rating scale "somewhat better" vs "no change") and distribution-based methods.
Results: The mean SF-6D score improved 0.050, from 0.705 ± 0.126 at baseline to 0.761 ± 0.131 at 12 months (P < .01). The mean EQ-5D score improved 0.060, from 0.810 ± 0.15 at baseline to 0.868 ± 0.15 at 12 months (P < .01). The ES (0.13-0.61) and SRM (0.13-0.57) were in the small-to-moderate range, demonstrating the responsiveness of the SF-6D and EQ-5D similar to other conditions. SF-6D and EQ-5D scores improved more for prolapse reconstructive surgical successes than for failures. The SF-6D and EQ-5D scores correlated with each other (r = 0.41; n = 645) and with condition-specific instruments. Correlations with the PFDI and PFIQ and their prolapse subscales were in the low to moderate range (r = 0.09-0.38), similar to other studies. Using the anchor-based method, the MID was 0.026 for SF-6D and 0.025 for EQ-5D, within the range of MIDs reported in other populations and for other conditions. These findings were supported by distribution-based estimates.
Conclusion: The SF-6D and EQ-5D have good validity properties and are responsive, preference-based, utility and general HRQOL measures for women undergoing surgical treatment for prolapse. The MIDs for SF-6D and EQ-5D are similar and within the range found for other medical conditions.
Keywords: EuroQol; Short Form 6D; health-related quality of life; minimal important difference; pelvic floor disorders; pelvic organ prolapse; utility score.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures

References
-
- Practice Bulletin No. 185: Pelvic Organ Prolapse. Obstet Gynecol 2017. November;130(5):e234–e250 - PubMed
-
- Drummond MF, Schulpher MJ, Torrance GW, O'Brien BJ, Stoddart GL. Methods for the Economic Evaluation of Health Care Programmes 3rd Edition ed. New York: Oxford University Press; 2005.
-
- Mehrez A, Gafni A. Quality-adjusted life years, utility theory, and healthy-years equivalents. Medical decision making : an international journal of the Society for Medical Decision Making. 1989;9(2):142–149. - PubMed
-
- Brooks R _EuroQol: the current state of play. Health Policy. 1996;37(1):53–72. - PubMed
