

Patient-Specific Multiscale Modeling of the Assisted Bidirectional Glenn
- PMID: 30471273
- PMCID: PMC6516076
- DOI: 10.1016/j.athoracsur.2018.10.024
Patient-Specific Multiscale Modeling of the Assisted Bidirectional Glenn
Abstract
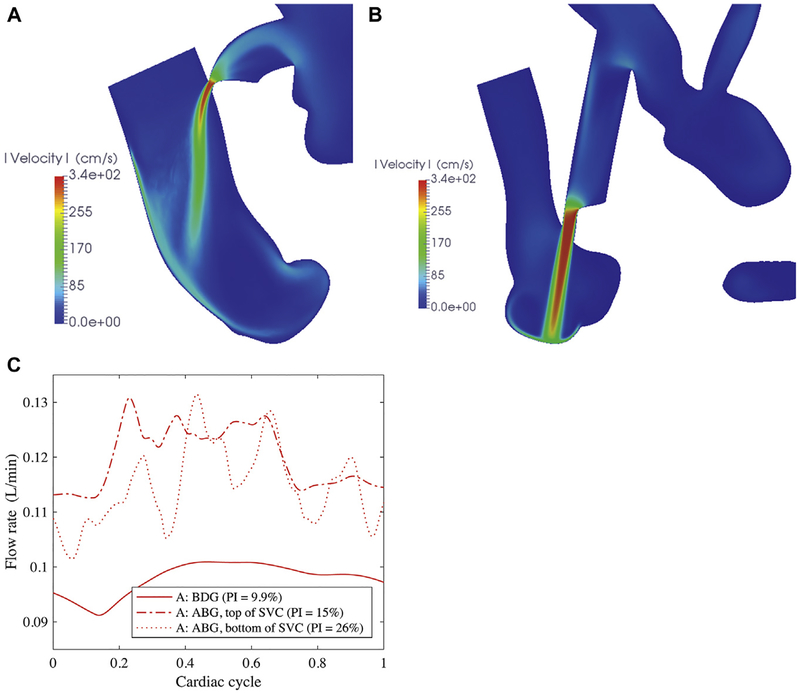
Background: First-stage palliation of neonates with single-ventricle physiology is associated with poor outcomes and challenging clinical management. Prior computational modeling and in vitro experiments introduced the assisted bidirectional Glenn (ABG), which increased pulmonary flow and oxygenation over the bidirectional Glenn (BDG) and the systemic-to-pulmonary shunt in idealized models. In this study, we demonstrate that the ABG achieves similar performance in patient-specific models and assess the influence of varying shunt geometry.
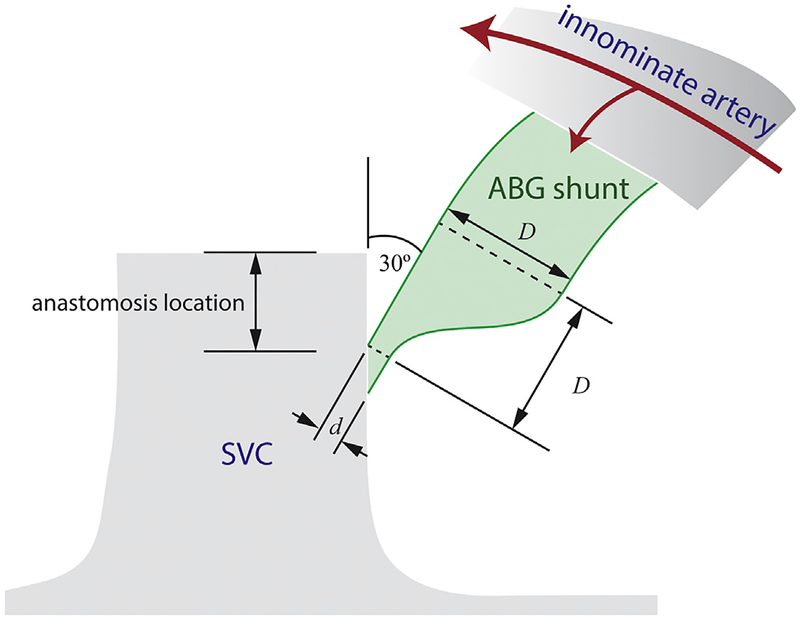
Methods: In a small cohort of single-ventricle prestage 2 patients, we constructed three-dimensional in silico models and tuned lumped parameter networks to match clinical measurements. Each model was modified to produce virtual BDG and ABG surgeries. We simulated the hemodynamics of the stage 1 procedure, BDG, and ABG by using multiscale computational modeling, coupling a finite-element flow solver to the lumped parameter network. Two levels of pulmonary vascular resistances (PVRs) were investigated: baseline (low) PVR of the patients and doubled (high) PVR. The shunt nozzle diameter, anastomosis location, and shape were also manipulated.
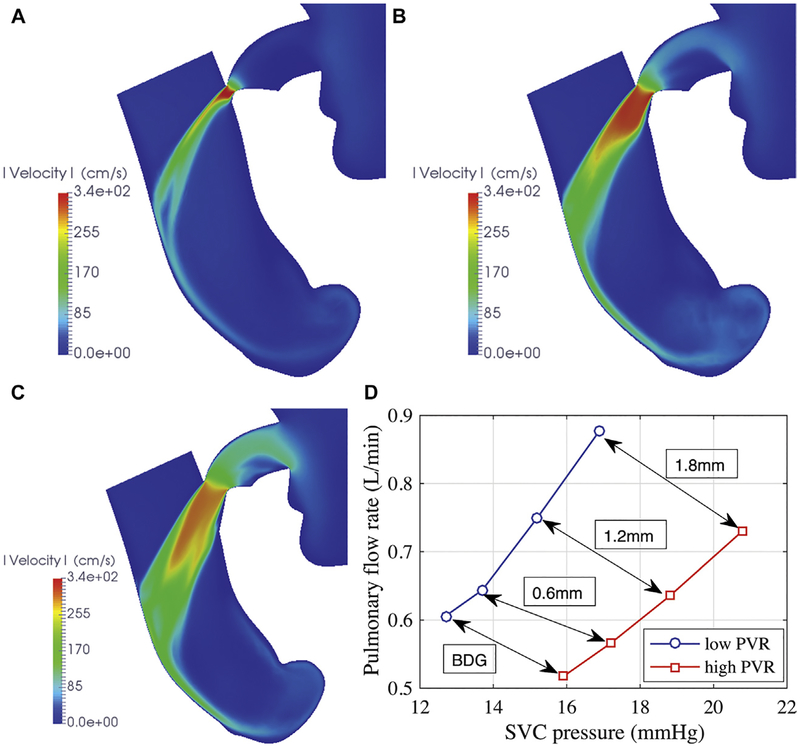
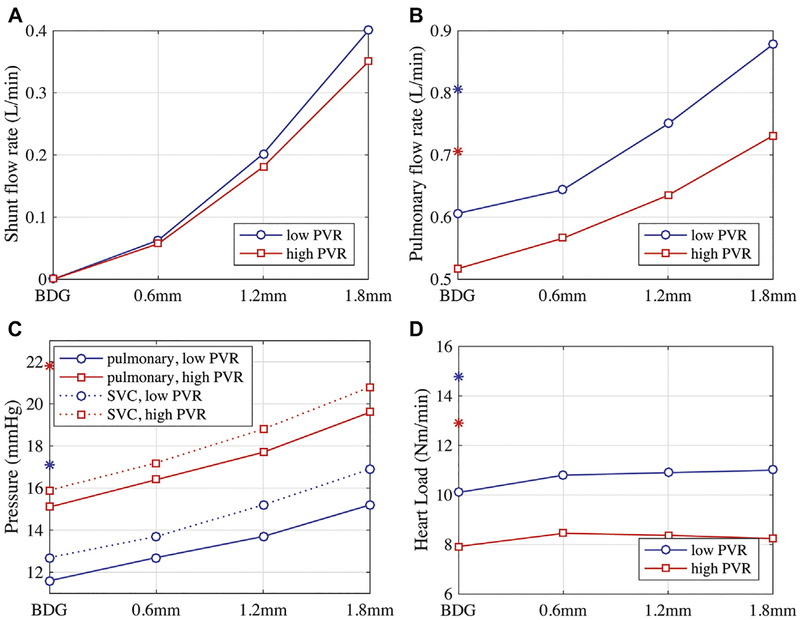
Results: The ABG increased the pulmonary flow rate and pressure by 15% to 20%, which was accompanied by a rise in superior vena caval pressure (2 to 3 mm Hg) at both PVR values. Pulmonary flow rate and superior vena caval pressures were most sensitive to the shunt nozzle diameter.
Conclusions: Patient-specific ABG performance was similar to prior idealized simulations and experiments, with good performance at lower PVR values in the range of measured clinical data. Larger shunt outlet diameters and lower PVR led to improved ABG performance.
Copyright © 2019 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited Commentary.Ann Thorac Surg. 2019 Apr;107(4):1239-1240. doi: 10.1016/j.athoracsur.2018.11.008. Epub 2018 Nov 24. Ann Thorac Surg. 2019. PMID: 30481518 No abstract available.
References
-
- Tamisier D, Vouhé PR, Vernant F, Leca F, Massot C, Neveux J-Y. Modified Blalock-Taussig shunts: results in infants less than 3 months of age. Ann Thorac Surg 1990;49:797–801. - PubMed
-
- Bartram U, Grünenfelder J, Van Praagh R. Causes of death after the modified Norwood procedure: a study of 122 postmortem cases. Ann Thorac Surg 1997;64:1795–802. - PubMed
-
- Glenn WW. Circulatory bypass of the right side of the heart, IV: shunt between superior vena cava and distal right pulmonary artery; report of clinical application. N Engl J Med 1958;259:117–20. - PubMed
-
- Glenn WW, Browne M, Whittemore R. Circulatory bypass of the right side of the heart: cava-pulmonary artery shunt—indications and results (report of a collected series of 537 cases) In: The Heart and Circulation in the Newborn and Infant. New York, NY: Grune & Stratton; 1966:345.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
