

Segmental Spinal Dysgenesis-"Redefined"
- PMID: 30472824
- PMCID: PMC6454287
- DOI: 10.31616/asj.2018.0076
Segmental Spinal Dysgenesis-"Redefined"
Abstract
Study design: Retrospective single institutional observational study.
Purpose: Segmental spinal dysgenesis (SSD), a complex spinal dysraphic state caused by notochord malformation disorders, is named after its morphological presentation where a spine segment is dysgenetic, malformed or absent. This study's objective was to examine and reassess SSD imaging findings and correlate them with an embryological explanation.
Overview of literature: Scott and his colleagues defined SSD as segmental agenesis or dysgenesis of the lumbar or thoracolumbar vertebrae and underlying spinal cord. Tortori-Donati and his colleagues defined it as a morphologic continuum ranging from hypoplasia to an absent spinal cord segment.
Methods: Fifteen children, whose imaging findings and clinical features were consistent with SSD, were included in the study. Magnetic resonance imaging (MRI) was performed per institutional spine protocol.
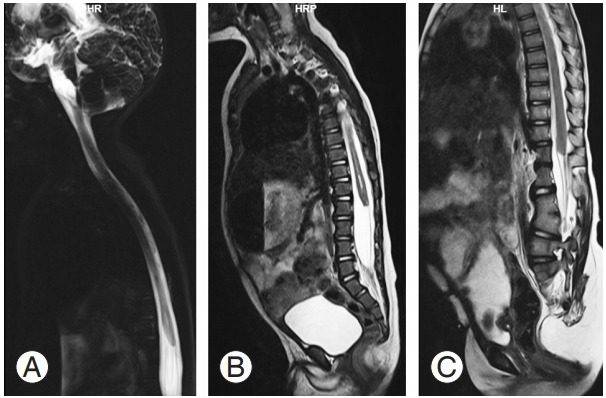
Results: Five children (33.3%) presented with a high-ending bulbous cord with no caudal segment, six (40%) presented with a dorsal or lumbar segmental dysgenetic cord with a low-lying, bulky caudal cord but without significant spinal canal narrowing, and four (26.6%) presented with segmental caudal dysgenesis with severe kyphoscoliosis, gibbus deformity, and spinal canal narrowing with a normal distal segment (normal or low-lying).
Conclusions: SSD is a complex spinal anomaly in children requiring clinical-radiological assessment followed by multidisciplinary management based on the extent and severity of the dysgenetic cord and the type of SSD. MRI plays a crucial role in both diagnosing and classifying SSD prior to surgical treatment to prevent further impairment.
Keywords: Magnetic resonance imaging; Scoliosis; Segmental spinal dysgenesis; Spinal cord.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures




References
-
- Scott RM, Wolpert SM, Bartoshesky LE, Zimbler S, Karlin L. Segmental spinal dysgenesis. Neurosurgery. 1988;22:739–44. - PubMed
-
- Bristol RE, Theodore N, Rekate HL. Segmental spinal dysgenesis: report of four cases and proposed management strategy. Childs Nerv Syst. 2007;23:359–64. - PubMed
-
- Zana E, Chalard F, Mazda K, Sebag G. An atypical case of segmental spinal dysgenesis. Pediatr Radiol. 2005;35:914–7. - PubMed
-
- Naidoo J, Mahomed N. Spinal segmental dysgenesis: case series. SA J Radiol. 2009;13:29–32.
LinkOut - more resources
Full Text Sources
Research Materials
