

Biochemical Analysis of Pleural Fluid and Ascites
- PMID: 30473591
- PMCID: PMC6223608
Biochemical Analysis of Pleural Fluid and Ascites
Abstract
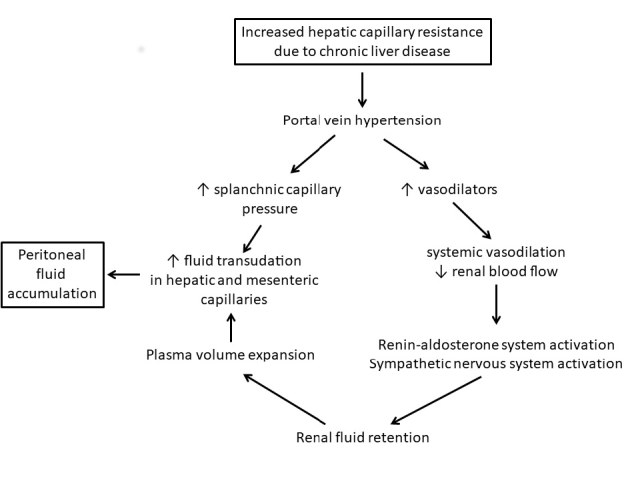
Biochemical testing of peritoneal and pleural fluids is carried out widely, although the range of tests likely to be useful is limited in comparison to the repertoire of tests available in a modern biochemistry laboratory. Fluids accumulate when pathological processes cause an imbalance between hydrostatic pressure gradients, capillary membrane permeability and lymphatic capacity, resulting in protein-poor transudates or inflammatory exudates. In peritoneal fluid, albumin is the most useful test, for the calculation of the serum-ascites albumin gradient; protein and LDH have a role regarding risk and diagnosis of spontaneous bacterial peritonitis and amylase may be useful in diagnosing fluid accumulation due to pancreatitis. Peritoneal fluid pH and glucose are not indicated analyses. For pleural fluid, protein and LDH are important in distinguishing between transudate and exudate using Light's criteria; albumin and the serum-effusion albumin gradient may have a complementary role in patients already on diuretics. Pleural fluid pH is the most useful marker of infection although LDH and glucose are also used. Pleural fluid amylase is often measured but, if raised, is more likely to reflect a malignant process than pancreatic disease as the former is much more prevalent. Tumour markers in both peritoneal and pleural fluids generally have limited diagnostic accuracy for detecting local malignancy. Limited studies validating standard serum test methods for use with pleural and peritoneal fluids have been published but work is progressing in this area both in Australasia and overseas and opportunities exist for contributing to this effort.
Conflict of interest statement
Competing Interests: None declared.
Figures
References
-
- Clinical and Laboratory Standards Institute. CLSI document C49-A. Wayne, PA, USA: 2007. Analysis of Body Fluids in Clinical Chemistry; Approved Guideline.
-
- Miserocchi G. Physiology and pathophysiology of pleural fluid turnover. Eur Respir J. 1997;10:219–25. - PubMed
-
- Siddall EC, Radhakrishnan J. The pathophysiology of edema formation in the nephrotic syndrome. Kidney Int. 2012;82:635–42. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical